
Part 1 – Evidence questioning the most widely held vaccine assumptions.
Part 2 – A look at a small fraction of the peer reviewed, published science which raises concerns about both vaccine efficacy and safety.
Part 4 – Examples of some apparently ineffective and/or unnecessary vaccines and consideration of the regulatory and licensing environment.
[Please Note: These articles form a single investigation. Reading them in order is recommended.]
![]()
The official need for the National Vaccine Injury Compensation Program (NVICP), according to the U.S. Health Resources and Services Administration (HRSA), is that lawsuits, “threatened to cause vaccine shortages and reduce vaccination rates.” This is both revealing and presents a contradiction.
 Firstly, if profit is a determining factor for vaccine availability then clearly we are looking at a business enterprise, not a public health program. Secondly, the number of lawsuits for vaccine injury are a contraindication, suggesting the need for caution. They are not a justification for maintaining ‘vaccine rates.’ Quite the opposite.
Firstly, if profit is a determining factor for vaccine availability then clearly we are looking at a business enterprise, not a public health program. Secondly, the number of lawsuits for vaccine injury are a contraindication, suggesting the need for caution. They are not a justification for maintaining ‘vaccine rates.’ Quite the opposite.
As I have tried to stress throughout this series, I am one among many who question some aspects of the official vaccination narrative. I do not reject vaccines outright and accept much of the scientific and medical evidence which clearly shows the public health benefit of some vaccines.
For example, the purified DPT (acellular) combined vaccine significantly reduced pertussis in young children, across Europe. It differed immensely from the cheaper DPT vaccine distributed in the U.S. which caused severe health harm for many infants.
This marked difference between two versions of the same vaccine illustrates the point I am hoping to make. Not all vaccines are created equal. Just because we have reason to value one doesn’t mean we should uncritically accept all. Especially in light of the growing vaccine schedule and increased use of combined vaccines.
The term ‘anti-vaxxer’ is being liberally applied to illegitimately silence criticism of some vaccines and the vaccine schedule. All part of the effort to convince an unquestioning public to accept mandatory vaccination.
“Anti-vaxxer” is just a label, used as a linguistic tool, to dismiss vaccine sceptics as science Luddites, cranks or dangerous agents of disinformation. This is done to ensure the vast majority, who apparently believe everything the media and the state tell them about vaccines, refuse even to look at the evidence prompting justifiable scepticism.
As we discussed previously, there is a plenty of historical, scientific and medical evidence to suggest the need for caution, especially given the increasing number with many more in the vaccine pipeline. This does not mean all those who highlight this information are entirely opposed to every vaccine. So you have to wonder why the state and the mainstream media keep insisting you believe that they are.
An Introduction To Vaccine Compensation Programs
We are going to focus largely upon the U.S. vaccine schedule because it is the most extensive in the world. However, the U.S. regulatory regime is broadly replicated in other developed nations. Surprising then that the U.S. only ranks 37th on the World Health Organisation’s population health league table. One below Costa Rica and 15 below Columbia. Obviously, vaccination rates are not a meaningful marker for overall quality of public health.
The U.S. National Vaccine Injury Compensation Program (NVICP) is managed by three separate U.S. government departments. The U.S. Department of Health and Human Services (HHS) hosts the program; the U.S. Department of Justice (DOJ) defends the HHS in the liability limited hearings and the U.S. Court of Federal Claims pays out, whatever it judges to be appropriate, if the DOJ lose.
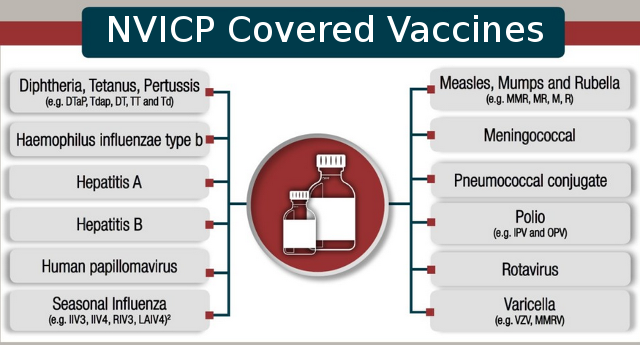
Since 1988 the NVICP has paid out $4.2 billion in compensation for people injured or killed by vaccines. The NVICP is funded by taxation, removing the burden of compensation completely from the shoulders of the pharmaceutical corporations and placing it entirely upon the tax payer.
Similar compensation funds exist elsewhere. In the UK the Vaccine Damage Fund (VDF), with a ceiling payout of just £120,000, has cost tax payers just over £74 million in compensation since 1978, for an estimated minimum of 1000 confirmed cases, representing about 12.5% of claims made. Similar Vaccine Injury Compensation (VIC) programs exist in 25 high income countries, mainly in Europe, the Western Pacific Region, North America and South East Asia. They are notably absent in middle to low income nations.
These VIC’s are overseen by the World Health Organisation’s (WHO) Global Vaccine Safety initiative. They were embroiled in the NPAFP vaccine scandal in India. The WHO are keen to stress the “no fault” element of the various VIC programs. They state:
“These programmes do not require injured parties or their legal representatives to prove negligence or fault by the vaccine provider, the health care system or the manufacturer before compensation. They serve to waive the need for accessing compensation through litigation…….All the no-fault VICPs reviewed require proof of a causal association between vaccination and injury……..As countries continue to extend the use of vaccines and strengthen their safety surveillance and investigative capacity, occasional severe vaccine-associated reactions will continue to be identified. No-fault VICPs are considered a measure to maintain confidence in immunization programmes.”
We can paraphrase this statement. VIC’s keep the pharmaceutical companies out of the courts. Once the claimant has proven the damage was caused by vaccination they must accept this is not the fault of either the state, public or private healthcare providers or the vaccine manufacturer before being eligible for any compensation. This is done to ensure the wider public believe all vaccines are perfectly safe, despite the evidence to the contrary.
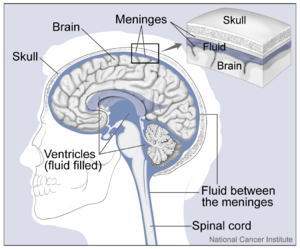
Most governments have acknowledged that vaccines cause a range of serious injuries. These include brain damage, seizure disorders, deafness, Guillain-Barré Syndrome (GBS), encephalitis (inflammation of the brain) and death. For example, in 1992 the MMR vaccine Pluserix was withdrawn from the UK vaccine market after it was found to cause aseptic meningitis.
Approximately 35% of the WHO’s annual budget of about $4.5 billion comes from non governmental organisations, philanthropic trusts and other non state partners. These partners include vaccine program profiteers the Bill & Melinda Gates Foundation, the vaccine manufacturers Merck, GlaxoSmithKline, Sanofi and Roche, among others, and a huge range of private healthcare, biomedical research and petrochemical corporations, such as Bayer AG. Whether the billions of dollars given to the WHO over recent years by these corporations had any bearing upon their 2019 definition of vaccine hesitancy as a global health threat is unknown.
Vaccines only provide a small percentage of Big Pharma profits but they are far from loss leaders. In 2017 the global Vaccine market was conservatively estimated to be worth $34.3 billion annually. The projected Compound Annual Growth Rate (CAGR) was around 7%. However, recent moves towards compulsory vaccination have seen market confidence soar.
With revenue projected to reach an estimated $77.1 billion per annum by 2024, an increased estimated CAGR of 10.3% is an attractive proposition for venture capitalists the world over. This growth is all but guaranteed providing as many people as possible are vaccinated. If mandatory vaccination extends to all adults then revenue will be measured in trillions not billions.
The pharmaceutical corporations can easily afford to pay the relatively small amount of compensation meted out by the likes of the NVICP and the VDF under the WHO compensation programs. So why are tax payers forced to cover their losses?
The Vaccine Balancing Act
 Both vaccinations and natural resistance to infection rely upon antigens in the bloodstream. Vaccine derived antigens (for a given pathogen) are introduced to stimulate lymphocytes to produce antibodies, providing subsequent immunity against contracting the pathogen (disease). Vaccination reduces the health risks associated with the disease itself by pre-programming the immune response before major infection . Conversely, it introduces the potential risk of vaccine harm.
Both vaccinations and natural resistance to infection rely upon antigens in the bloodstream. Vaccine derived antigens (for a given pathogen) are introduced to stimulate lymphocytes to produce antibodies, providing subsequent immunity against contracting the pathogen (disease). Vaccination reduces the health risks associated with the disease itself by pre-programming the immune response before major infection . Conversely, it introduces the potential risk of vaccine harm.
Natural infection avoids possible vaccine injury but runs the increased risk of contracting the disease. The child is more likely contract the pathogen and thereafter “self-antigens” bind to the antibodies to fight the infection. However, the level of immunity following natural infection is generally longer lasting than that provided by vaccines. Though this will depend upon the disease and the immune system of the infected person.
This used to be well known by parents. Hence the MMR parties of a few years ago, where children’s highly adaptable immune systems would be deliberately exposed to infection. This was done to hopefully avoid the known higher risk associated with contracting the same disease later in life. When an entrenched, less flexible adult immune system tends to cause additional complications.
To illustrate, in 2014 researchers noted the waning effectiveness over time of the varicella vaccination in the U.S. population. This had greatly reduced incidents of childhood chicken pox but had coincided with a significant increase the much more serious adult varicella disease of shingles. On balance, in light of both the health impacts and care costs of treating shingles in adults, the researchers concluded:
“….the universal varicella vaccination program is neither effective nor cost-effective.”
Parental Choice?
Every parent need to make a risk assessment prior to vaccinating their child. Should they refuse and expose their child to natural infection, aiming for a greater chance of life long immunity, or vaccinate, reducing the immediate risk while potentially increasing the likelihood of poorer adult health? Additionally, parents need to know the chances of serious childhood illness, following infection, balanced against the odds of a harmful reactions to vaccine.
Many people are actively campaigning to take that choice away from parents. Giving more control of a child’s health to the state. Regardless of the vaccine debate, is it tenable to believe the state will care for a child as a loving parent would? The State’s track record in this regard is appalling.
To inform this vaccination decision parent need access to clear, honest, unbiased information. Unfortunately, as we shall she, the vast majority of promoted vaccine information is not trustworthy and major conflicts of interest permeate the vaccine information made available to the public.
In 1955 in the U.S. 200 people were paralysed and 10 died after receiving the Salk Polio vaccine. The liability for compensation stemming from the law suits that followed, fell upon the manufacturer Cutter Laboratories. During the 70’s and 80’s a similar slew of court cases followed the serious injuries caused by the DPT vaccine. A safer “acellular” variant was available which greatly reduced the health risks, but it was considerably more expensive. While many countries opted for this purified version, in the U.S. the Center for Disease Control and Prevention (CDC) chose not to use the safer variety, with devastating effects.

A 1977 a study by Dr. Gordon T. Stewart, of the Department of Community Medicine at the University of Glasgow, found that 1 of every 54,000 DPT vaccinated children contracted encephalopathy (brain disfunction) amid a range of other neurological and physiological disorders. The litigation which followed in the U.S. threatened to bring vaccine manufacturing to a halt. The pharmaceutical corporations were unable to insure their liabilities and their profit margins dwindled. By 1984 many U.S. based corporations had left the vaccine market. Pharmaceutical corporation sell drugs for profit. There is no commitment to public health.
In response to this the U.S. Government passed the 1986 National Childhood Vaccine Injury Act (NCVIA), establishing the Vaccine Adverse Event Reporting System (VAERS), which we’ll discuss shortly. The NVICP followed in 1988, removing any fears of liability from the vaccine manufacturers.
In his study Dr. Stewart noted that adverse events were severely under-reported or overlooked and recognised he was unable to identify the level of protection against pertussis claimed by the substandard DTP vaccine manufacturer. The question he asked was quite simple. Do the health benefits of a particular vaccine outweigh the assessed risk of harm caused by it?
This hardly seems contentious. Surely this is central to the precautionary principle? And yet, in the current media polluted atmosphere surrounding vaccines, asking this question labels you an “anti-vaxxer.” Of more concern, health policy makers, scientists and medical practitioners aren’t asking themselves this same question. For our purposes, let’s call them the PSM.
The immediate retort to this will be that the PSM are cognizant of this consideration, that all vaccines are perfectly safe and only stupid ‘anti-vaxxers‘ would even raise this issue. However, for a number of vaccines, that assumption is false.
 To answer the question, certain prerequisites need to be met. Firstly you need to have reliable data on the effectiveness of the vaccine. You need to know precisely how infection rates and the symptoms are improved by vaccination. How, and to what specific extent, does administering a particular vaccine deliver better health outcomes than ordinary, natural infection, where infection rates have reduced anyway due to other public health improvements? As the vaccine schedule has rapidly expanded, you also need to understand the risks and benefits for the cumulative effect of administering many more vaccines, often in combination and in a relatively short time frame.
To answer the question, certain prerequisites need to be met. Firstly you need to have reliable data on the effectiveness of the vaccine. You need to know precisely how infection rates and the symptoms are improved by vaccination. How, and to what specific extent, does administering a particular vaccine deliver better health outcomes than ordinary, natural infection, where infection rates have reduced anyway due to other public health improvements? As the vaccine schedule has rapidly expanded, you also need to understand the risks and benefits for the cumulative effect of administering many more vaccines, often in combination and in a relatively short time frame.
Secondly you need to know, with a considerable degree of accuracy, what the adverse reactions are, their severity and prevalence. Without this data you simply cannot know if the vaccine risks are acceptable compared to the known risk of disease.
Unfortunately, the PSM tasked with providing vaccine cover for the population don’t have a clear picture of this data. They are not questioning either vaccine efficacy or safety. Those who do are ostracized and attacked for ever doubting vaccines. For a number of scheduled vaccines, efficacy and safety are just assumed with little to no substantiating evidence, particularly in regard to the scheduled mixing of both monovalent and combined vaccines.
Problems With Establishing Vaccine Effectiveness (VE)
In the U.S, in the first 18 years of life, children are injected with a total of 72 doses of various vaccines supposedly improving their health outcomes. They receive 28 doses before their second birthday. This is based upon the total number of doses not shots, as it includes combined vaccines such as MMR and DTaP (counting each shot as 3 doses.) Counting doses in this way is consistent with U.S. Government taxation of vaccines, which funds the NVICP. This tax is levied per dose, meaning one shot of MMR is counted as three doses.
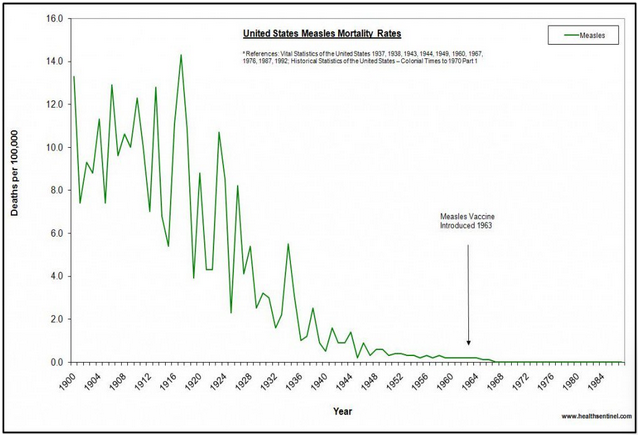
Claims that vaccines are solely responsible for the significant decline in disease seen in the 20th century fail to acknowledge the considerable impact of other public health improvements, such as the widespread adoption of the Leicester Method. For example, it is claimed that measles mortality in the U.S. was eradicated by the measles vaccine. This claim is dubious. Measles mortality was near to zero before vaccines were introduced in 1963. The measles vaccine undoubtedly further reduced mortality rates but, absent the accompanying broader public health improvements, there is no evidence the measles vaccine alone was responsible for the claimed eradication.
The only way to clearly establish vaccine efficacy (VE) today is by comparing the health outcomes of vaccinated populations against those of the unvaccinated, where public health standards are equivalent for both groups.
There are no officially acknowledged long term, large scale studies comparing the health outcomes of those who follow the U.S. vaccination schedule against those who don’t (the unvaccinated). The broad comparative health benefits of injecting this combination of 72 doses, throughout infancy and adolescence, are not clearly understood. Or rather, they aren’t acknowledged.
There are a few studies from other countries which attempt to make large scale comparison between the vaccinated and unvaccinated. Each have different vaccine schedules using different types and brands of vaccines, so no direct correlation can be made with other national vaccine schedules.
A 2011 study by German researchers looked at the comparative health outcomes of nearly 18000 children. It found greater resistance to infection among the vaccinated child population:
“The proportion of children and adolescents who had had pertussis, measles, mumps, and/or rubella was much higher in unvaccinated children than in those who had been vaccinated against the respective disease.”
However, they also discovered the vaccinated had higher infection rates for diseases not on the vaccine schedule. Using median analysis of the 1-5yr group the unvaccinated contracted 3.3 ‘non preventable diseases’ while the vaccinated infants contracted 4.2 on average. Among 11- to 17-year-olds, the corresponding figures were a median average of 1.9 (unvaccinated) versus 2.2 (vaccinated). From a VE perspective this suggests that vaccination reduces overall natural immunity. Though the researchers stated they did not think this significant.
The study also shows, contrary to some of the more outlandish claims of vaccine supporters, vaccination doesn’t stop children becoming infected with ‘preventable diseases’. It reduces the chances of infection. It is therefore very difficult to see how vaccines alone can eradicate diseases. As discussed earlier in this series, other public health factors must also play a part in the near eradication of some diseases. The question is, to what extent.
This more complex picture was acknowledged by another large scale 2015 comparative study of the impact of vaccines in Malawi in East Africa. It wasn’t feasible to quantify VE. The compounding factors, such as distance from vaccine centers, poverty, poor sanitation, overcrowding etc were inextricably linked to disease rates. It was near to impossible to derive a clear methodology for evaluating VE.
Such environmental factors are still relevant, to a lesser extent, in developed nations. For example, the vast majority of us have access to clean drinking water but housing condition vary greatly.
This may explain why, in the 2012 Congressional hearing on autism before the House Committee on Oversight and Government Reform, Dr. Coleen Boyle, then Director of the CDC’s National Center on Birth Defects and Developmental Disabilities stated:
“We have not studied vaccinated versus unvaccinated [children].”
There haven’t been any reliable large cohort comparison studies since. Consequently, there is very little evidence to demonstrate VE for the U.S. vaccine schedule. This is echoed in the UK and many other developed nations, whose own vaccine schedules are equally lacking any reliable large scale comparative cohort studies.
Despite risible ‘nothing to see here‘ stories spewed out by the MSM, the problem of multinational corporations funding scientific research, invariably proving their own products are brilliant, is a major factor contributing towards a genuine crisis in science. With regard to vaccine efficacy research, this problem has been long known. In 2009 a research team from the respected Cochrane Colaboration wrote a paper on the impact of corporate finance on published influenza vaccine science.
 They looked at papers written about the influenza vaccine. In particular they were looking to see if the data within the paper supported the conclusion. The more accurately the data evidenced the conclusion, the higher the ‘concordance.’ They compared this with the funding sources of the paper. 48% Were government funded, 29% declared corporate funding and 23% didn’t say where their funding came from.
They looked at papers written about the influenza vaccine. In particular they were looking to see if the data within the paper supported the conclusion. The more accurately the data evidenced the conclusion, the higher the ‘concordance.’ They compared this with the funding sources of the paper. 48% Were government funded, 29% declared corporate funding and 23% didn’t say where their funding came from.
While 70% of studies were favourable to the vaccines, only 18% showed solid concordance between the data reported and study conclusions. Over half (56%) were considered at high risk of bias and only 4% were considered low risk. Greater concordance was attributed to better methodology, not funding levels. The study concluded:
“……the higher the probability of concordance, the lower the probability that a study’s conclusions were in favour of vaccines’ effectiveness….”
In other words, the concordance (quality) of the paper was considerably higher for the 30% of papers questioning vaccines that the 70% extolling their virtue. Due to the high proportion of unknown funders the study couldn’t clearly state to what extent industry funding skewed the conclusions in the papers analysed. However, they stated:
“…..there was an inverse association between conclusions in favour of the vaccines’ effectiveness and government funding, This finding confirms the established association between funding source and type of study conclusions.”
Meaning a disproportionate number of poorer quality vaccine favourable papers were funded either by pharmaceutical corporations or unknown financiers. The Cochrane researchers found a clear correlation between corporate funding and the publication of those papers in prestigious journals.
“Publication in prestigious journals is associated with partial or total industry funding, and this association is not explained by study quality or size.”
Cochrane also looked at how often those published papers were cited by others as evidence. They scored the papers based upon the frequency of their citation. They found the studies less favourable to vaccines had a citation score of 3.74 compared to 8.78 for industry funded studies favourable to vaccines.
What this shows is that the influenza vaccine efficacy papers, published in the most prestigious medical journals, were predominantly funded by pharmaceutical corporations. These papers were at high risk of bias and were of generally poor quality, lacking concordance. However, they were far more likely to be referenced as evidence by others.
The researchers noted the likely impact of this on medical professionals. They recognised that professionals, hoping to stay informed about medical advances, rely heavily upon the so called prestigious journals. Pressed for time, research shows, that most simply read the conclusions, trusting the supposed integrity of the publisher and wrongly assuming they had done their due diligence on the evidence presented before publishing the paper.
In 2009 this meant that GP’s and paediatricians were largely reading poorly evidenced pap, advocating biased industry funded vaccine research, before advising parents on the efficacy of those same vaccines. Parents, trusting the advice of Doctors, who were in no way deliberately misleading them, were given poor quality advice about influenza vaccine effectiveness.
Not only is there a distinct lack of large comparative cohort studies demonstrating VE, the guidance, filtered down to parents, in order to inform their decision, was also questionable. Ten years later their is no evidence to suggest anything has changed.
Problems With Establishing Vaccine Safety (VS)
Just as with establishing VE, determining vaccine safety (VS) is equally complex. In general vaccine risks are measured by analysis of injury claims and reported vaccine injuries. There are considerable problems with the collection and analysis of this data. Other issues with verifying data include unreliability due to conflict of interest, poor methodology and unexplained omission.
 Recently the Guardian, in an woefully uncritical example of alleged journalism, confidently reported that there was no link between the MMR vaccine and Autism. This was based upon an large cohort comparative study by Danish researchers. It was also cited by numerous health care providers, including the NHS in the UK. What the media and compliant health services neglect to mention is that this study was practically written by the pharmaceutical corporations.
Recently the Guardian, in an woefully uncritical example of alleged journalism, confidently reported that there was no link between the MMR vaccine and Autism. This was based upon an large cohort comparative study by Danish researchers. It was also cited by numerous health care providers, including the NHS in the UK. What the media and compliant health services neglect to mention is that this study was practically written by the pharmaceutical corporations.
Three of the study’s authors worked for the Statens Serum Institut, a profit making Danish vaccine manufacturer and distributor, and the research was funded by the Danish multinational pharmaceutical corporation Novo Nordisk. Why neither the Guardian nor the NHS felt the public needed to know anything about this is hard to say. But it certainly doesn’t lend much credibility to the either the study or their reporting of it.
Those who accuse people of being ‘anti-vaxxers’ will say just because a pharmaceutical corporations funds a study, it doesn’t mean it is biased. The same could be said for the studies they published claiming Thalidomide was safe. To avoid jumping to conclusions is wise, but to ignore precedent and deny the high probability of bias is stupid.
Yet, despite the difficulties and prominent denials, the CDC seemingly did conduct large comparative cohort studies on vaccine safety in the late 1990’s. The CDC maintain a database called the Vaccine Safety Datalink (VSD). It records statistical data of vaccine related injuries. This used to be openly searchable by the public but now you need CDC permission.
In 1999, based upon his analysis of the VSD, Dr. Thomas M. Verstraeten produced a study called “Increased Risk Of Developmental Neurologic Impairment After High Exposure To Thimerosal-Containing Vaccine In First Month Of Life.” He analysed the medical history of 400,000 infants born in the U.S. between 1991 and 1997. Narrowing his focus upon the Thimerosal adjuvant in the HepB vaccine, Verstraeten compared the health outcomes of the vaccinated against the unvaccinated.
The risk of developing autism for the vaccinated children was 7.6 times greater than for the unvaccinated. He continued to analyse the data, recording the following comparisons:
- Children given the Hep B vaccine were 5 times more likely to suffer sleep disorders,
- They were more than twice as likely to have speech disorders
- The HepB vaccinated were nearly twice as likely to have neurodevelopmental disorders.
This raised some concerns and, in September 2000, a meeting was convened by CDC’s Epidemic Intelligence Service, at Simpsonwood Retreat Centre in Georgia. The transcript of that meeting illustrates the CDC were focused upon protecting against litigation and burying the results.
The CDC’s approach was not universally shared by the paediatricians present at the meeting. Many were more concerned about the welfare of children. Dr. William Weil, representing the American Academy of Pediatricians, said:
“There are just a host of neurodevelopmental data that would suggest that we’ve got a serious problem……To think there isn’t some possible problem here is unreal……The number of dose related relationships are linear and statistically significant. You can play with this all you want. They are linear. They are statistically significant.”
Other medical professionals present were less worried about children. Dr. Robert Brent, a scientific advisor for the American Council on Science and Health, was far more concerned about the risk of litigation. He said:
“The medical/legal findings in this study, causal or not, are horrendous……you could readily find junk scientist who would support the claim with a reasonable degree of certainty…….you will not find a scientist with any integrity who would say the reverse with the data that is available…….So we are in a bad position from the standpoint of defending any lawsuits if they were initiated and I am concerned.”
Dr. Roger Bernier, Associate Director for the CDC’s National Immunisation Program, added:
“We have asked you to keep this information confidential….Consider this embargoed information.…and very highly protected information”
 This seeming policy of evidence obfuscation and denial was reinforced in court by the U.S. Department of Justice in the 2007 Omnibus Autism Proceedings (OAP). They found the vaccine causation claims of 5600 families ‘untenable’ and refused to pay any damages.
This seeming policy of evidence obfuscation and denial was reinforced in court by the U.S. Department of Justice in the 2007 Omnibus Autism Proceedings (OAP). They found the vaccine causation claims of 5600 families ‘untenable’ and refused to pay any damages.
Dr. Andrew Zimmerman was due to testify as an expert witness on behalf of the HHS in the OAP. He had previously written a statement for the court in reference to separate case of one of his patients. In that case he said there was no evidence of a causal relationship between the MMR vaccine and her autism diagnosis. This was written solely for her case, not the OAP hearings. Realising his statement was being used in the OAP hearings as evidence disproving any link between vaccines and autism, Dr. Zimmerman protested to the DOJ lawyers and stated:
“….there were exceptions in which vaccines could cause autism…..in a subset of children with an underlying mitochondrial dysfunction….in at least one of my patients, did cause regressive encephalopathy with features of autism spectrum dissorder.”
Having raised his concerns the DOJ lawyers struck Dr Zimmerman off their list of expert witnesses and his testimony wasn’t heard in the OAP hearings.
Today, 20 years after Dr. Verstraeten’s research paper, the CDC state on their website:
“There is no evidence of harm caused by the low doses of thimerosal in vaccines, except for minor reactions like redness and swelling at the injection site.”
Thimerosal (an ethyl Mercury compound) remains an adjuvant in the influenza vaccine. This is given to millions of adults around the world every year and is also routinely recommended for administration to infants and pregnant women to ‘protect them.’
Meanwhile, rates of autism spectrum disorders (ASD) have skyrocketed. Between 2000 and 2014 U.S. rates of diagnosed ASD grew from and estimated 1 in 150 children in 2000 to an estimated 1 in 40 by 2016. Suggesting above a 350% increase in less than two decades. The first live attenuated influenza vaccine (LAIV) was approved by the U.S Food and Drug Administration in 2003.
While no one has any idea at all why this increase has occurred we are told it definitely isn’t anything to do with vaccines. A myriad of explanations have been offered. From better diagnostics (350% improved in just 16yrs) to global warming. Every avenue has been explored but only vaccines have been discounted as a potential cause.
This all seems rather odd, given the CDC’s own suppressed analysis of the VSD suggested a link. As do many other peer reviewed scientific research papers.
In 2014, this prompted a team of U.S. university researchers to analyse the 6 papers the CDC cherry picked to substantiate their view that introducing ethyl Mercury compounds directly into the bloodstream of pregnant mothers and infants was perfectly safe. They concluded:
“There are over 165 studies that have focused on Thimerosal…….[which] found it to be harmful….The studies upon which the CDC relies and over which it exerted some level of control report that there is no increased risk of autism from exposure to organic Hg in vaccines…..These six studies are in sharp contrast to research conducted by independent researchers over the past 75+ years that have consistently found Thimerosal to be harmful…..Thimerosal has been found to be a risk factor in speech delay, language delay, attention deficit disorder, and autism…..Importantly….. five of the publications examined in this review were directly commissioned by the CDC, raising the possible issue of conflict of interests or research bias, since vaccine promotion is a central mission of the CDC.”
[Note: Bracketed information added]
 The CDC isn’t remotely independent of the pharmaceutical corporations. In 1990’s the U.S Government created a number of ‘non profit’ foundations for government agencies, such as the CDC and the Food and Drug Administration (FDA). Senior Vice President of the Lowe Institute Shannon Brownlee noted:
The CDC isn’t remotely independent of the pharmaceutical corporations. In 1990’s the U.S Government created a number of ‘non profit’ foundations for government agencies, such as the CDC and the Food and Drug Administration (FDA). Senior Vice President of the Lowe Institute Shannon Brownlee noted:
“The foundations exist at least in part because they allow industries to directly fund and thus control the work of agencies that are either supposed to regulate them, or conduct research that can help or hurt their business.”
A quick look at the CDC Foundations partners reveals who is funding their programs. GlaxoSmithKline, probably the largest single vaccine manufacturer in the world, contribute, as do many of their global corporate competitors. Merck, Sanofi, Novavax, Emergent BioSolutions, CSL and Bavarian Nordic all willingly give their financial support to the CDC.
This has absolutely no influence at all on anything the CDC does and every decision they make is entirely unbiased, open, honest and transparent. It is up to you to decide if you think the previous sentence is plausible.
Where Does This Leave Parental Choice?
Ultimately this corporate pollution of vaccine ‘facts’ available to parents makes it extremely difficult for them to judge which vaccines they wish their children to receive. The evidence for both the efficacy and safety of some is far clearer than for others. Similarly doctors, upon whom parents generally rely for advice, face problems in weeding out the biased and profit driven science from the more reliable, genuinely independent studies.
Unfortunately, publication in allegedly reputable medical journals no longer signify either study quality or due diligence on behalf of the publisher. Like parents, doctors need to look beyond the more widely publicised vaccine studies if they hope to provide the best possible advice. For both parents and professional this would require a significant time commitment. One limited by the demands of busy working lives.
Yet the alternative is simply to rely upon whatever the media report, politicians say or the findings of industry funded studies. It is naive to imagine the vast sums involved have no impact upon vaccine information in the public domain. Especially in light of the huge increase in predicted revenue if mandatory vaccination is legislated.
What’s worse is the undeniable nexus between the the mainstream media, the political establishment and the pharmaceutical corporations which vilifies and, when necessary, destroys anyone who openly questions vaccines. This is the antithesis of both scientific inquiry and open, honest discourse. We should all ask ourselves why those who seek to silence debate fear it.
In the final Part 4 of the series we’ll look at the how vaccines are licensed. We will also consider some shocking evidence which raises serious concerns about a number of vaccines currently available on both the U.S. and European vaccine schedules.





The drug toxicity is never discussed. In fact this indusry ignores that the ony purpose of the adjuvant is to get a reaction which is the human bodies natural immune response to a toxin. i.e. [diarrhea, dizziness, nausea, stomach pains, vomiting, and weakness. More severe symptoms can include hand tremors, ataxia, muscle twitches, slurred speech, nystagmus, seizures, coma and, in rare cases, heart problems].[Verywell Mind]. These reactions are then claimed as the vaccine is successful because it created a reaction.
Most governments have acknowledged that vaccines cause a range of serious injuries. Why do they continue to protect this industry. Qui Bono?
Thanks John. I think multinational corporations and government are indivisible. They are two components of the same global order.
Dude,
You’re an awesome writer and I don’t say that lightly. Really well thought out, articulate. The contrast to the other side is ridiculous. I just watched “Vaxed” again and was reading the comments and they’re at this level..Paraphrased
“Total propaganda garbage…I didn’t watch the movie, and I wouldn’t because it’s just shit”
I’m not even exaggerating several people admitted, and others implicated by their ignorance that they Didn’t Even Watch The Movie but were able to offer similar critical insights.
What’s happened to people? Are they already under mind control, or are there that many truly evil people now? And speaking of Evil, somewhere in there is where I read a comment and then a call out against Dr Mercola and 11 other Frontline Doctors and/or Health (Freedom?) Providers by the CDDH, which shocked me, and that’s how I got to you.
I had to research who those crazy anti-anti-Hate fucks were and one of the first articles I read was part 1 of yours. Excellent job, worst Anti-Haters ever, maybe. Advocated assembling anti-terror, nuclear strike force teams against those super violent anti-vaxxer types.
Thanks Dick. I don’t think the majority of people are evil but we have all perhaps too easily forgotten how important critical thinking and asking questions of power is.