
[IMPORTANT Correction: The original version of the article stated that researcher Fran Leader questioned Pfizer. In fact her email exchange was with the MHRA.]
COVID 19 vaccine trials appear to have caused some confusion. Hopefully, this article might help clear things up a bit. People genuinely appear to believe that the COVID 19 vaccines have undergone clinical trials and have been proven to be both safe and effective. That belief is simply wrong.
The main point is this. If you decide to have Pfizer and BioNTechs experimental mRNA-based BNT162b2 (BNT) vaccine, or any other claimed COVID 19 vaccine for that matter, you are a test subject in a drug trial.
The mRNA in the BNT vaccine was sequenced from the 3rd iteration of the original WUHAN published Genome SARS-CoV-2 (MN908947.3). However, the WHO protocols Pfizer used to produce the mRNA do not appear to identify any nucleotide sequences that are unique to the SARS-CoV-2 virus. When investigator Fran Leader questioned the UK Medicines and Healthcare Products Regulatory Agency (MHRA) they clarified what the Pfizer vaccine was not based upon:
“The DNA template does not come directly from an isolated virus from an infected person.”
Nor are there any completed clinical trials for these vaccines. Trials are ongoing. If you are jabbed with one, you are the guinea pig. This may be fine with you but it’s not a leap of faith I or my loved ones wish to take. However, everyone is different.
On December the 8th the BBC reported a study in the Lancet and categorically stated:
“The Oxford/AstraZeneca Covid vaccine is safe and effective, giving good protection, researchers have confirmed”
The BBC had no justification to make this claim. The study in the Lancet did not confirm anything of the sort. The researchers wrote:
“ChAdOx1 nCoV-19 has an acceptable safety profile and has been found to be efficacious against symptomatic COVID-19 in this interim analysis of ongoing clinical trials.”
This was an interim analysis funded by, among others, CEPI and the Bill and Melinda Gates Foundation. The analysis was based upon trials which are years from completion and haven’t reported anything. The researchers also stated:
“There were no peer-reviewed publications available on efficacy of any severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines…”

There is no clear scientific evidence establishing either the safety or efficacy of proposed COVID 19 vaccines. The BBC and other MSM reports that this evidence exists are false.
We are going to focus on Pfizer and BioNTech’s BNT vaccine but all the manufacturers have essentially exploited the same trick. The regulators and governments have worked with the pharmaceutical corporations to conflate the limited data from the initial, or phase one, trials with the incomplete and ongoing data collection from the substantially larger phase two and three trials. The MSM have then falsely claimed the 1,2,3 phase trials are complete and insinuated that the untested data demonstrates vaccine efficacy and safety.
In reality, not only has the reporting of existing data been manipulated to show efficacy that isn’t evident in the raw data itself, the most important and meaningful phases of the trials have barely begun, let alone been completed.
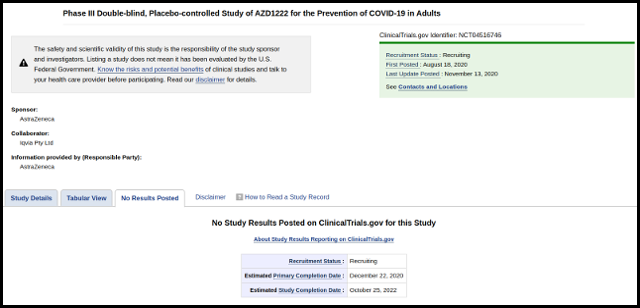
Recently the UK Financial Times reported that the UK regulators (the MHRA) are due to approve Astrazeneca/Oxfords AZD1222 [ChAdOx1] COVID 19 Vaccine. The FT revealed an anonymous statement from the UK Department of health:
“The medicines regulator is reviewing the final data from the University of Oxford/AstraZeneca phase 3 clinical trials to determine whether the vaccine meets their strict standards of quality, safety and effectiveness.”
Thus giving the public the impression that the trials are complete and that the regulators have strict safety standards. The 1,2,3 phase trial for AZD1222 was registered with the U.S. Centre for Disease Control as clinical trial NCT04516746 [Archived 29th December 2020]. It is incomplete and the estimated end date is February 21st 2023. The CDC state:
“No Study Results Posted”
Astrazeneca are years away from reporting any “final data.” It is impossible for the UK Department of Health to review it, because it doesn’t exist.
NCT04516746 is one of four trials of AZD1222. Another Russian arm of the AZD1222 trial was suspended after a Suspected Unexpected Serious Adverse Reaction (SUSAR) event occurred. The SUSAR supposedly happened in the United Kingdom after a 37 year old women developed inflammation of the spinal cord. It appears the Russian Ministry of Health have yet to reinstate their arm of the Astrazeneca/Oxford trial while it has resumed in the UK and elsewhere.
What Vaccine Trials?
On November 18th Pfizer and BioNTech announced they had concluded their phase three trial of BNT. They had demonstrated efficacy of 95% and U.S. Food and Drug Administration’s (FDA’s) Emergency Use Authorization (EUA) safety data milestone had been met.
 The only part of this claim that was true was compliance with FDA emergency safety data milestones. They have not concluded their phase three trials. They haven’t even fully completed phase one.
The only part of this claim that was true was compliance with FDA emergency safety data milestones. They have not concluded their phase three trials. They haven’t even fully completed phase one.
Under section 564 of the Federal Food, Drug, and Cosmetic Act (FD&C Act) so called “unapproved” drugs are allowed on the market in emergencies. Similarly, in the UK, authorisation under Regulation 174 of the Human Medicine Regulations 2012 (as amended) permits the same.
Having also been approved in the UK, this is why the Medicines and Healthcare products Regulatory Agency (MHRA) state:
“This medicinal product does not have a UK marketing authorisation”
The fact that there are no completed clinical trials for the Pfizer and BioNTech BNT vaccine also explains why the FDA State:
“Additional adverse reactions, some of which may be serious, may become apparent with more widespread use of the Pfizer-BioNTech COVID-19 Vaccine.”
The FDA also noted:
“[There is]…currently insufficient data to make conclusions about the safety of the vaccine in sub-populations such as children less than 16 years of age, pregnant and lactating individuals, and immunocompromised individuals…..[the] risk of vaccine-enhanced disease over time, potentially associated with waning immunity, remains unknown.”
Yet the first people to receive this vaccine are the most vulnerable in society, many of whom are immunocompromised. The precautionary principle appears to have been abandoned. The notion that the purpose of the BNT vaccine roll out is to save life appears untenable.
The Pfizer announcement enabled politicians to pretend to cry on national television while others were really excited. UK Prime Minister Boris Johnson said it was “fantastic news,” and the BBC said it was “good news” and “really encouraging.” Everyone was thoroughly impressed with the 95% effective claim.

However, this was based upon relative risk reduction. That is the declared percentage difference between the vaccinated group’s 8/18310 chance (0.044%) of developing COVID 19 against a 162/18319 (0.88%) chance of COVID 19 symptoms without the vaccine. As this larger group of 43,000 people have yet to be trialled, there is no basis for this claimed outcome. But it is what it is, and we can use these reported figures here.
It should be noted this only refers to an alleged reduction of COVID 19 symptoms among those who have the virus. The tested endpoints do not demonstrate that the vaccine will either reduce the spread of infection or save lives. It should also be noted that these figures suggest the threat from COVID 19 is vanishingly small.
Using Pfizer’s figures, the relative risk reduction is 100(1 – (0.044/0.88)). Which is 95%. Voila!
This sounds fantastic and is a much better marketing strategy than reporting the absolute risk reduction. The absolute risk of developing COVID 19 symptoms without the vaccine is supposedly 0.88% and with the vaccine 0.044%. In absolute terms, the effectiveness of the vaccine is (0.88-0.044)%.
A risk reduction of approximately 0.84%. Oh! A barely perceptible “efficacy.”
By using the relative instead of absolute risk reduction, the mainstream media (MSM) were free to market the mRNA vaccine for Pfizer and BioNTech (and other interested parties) with impressive sounding claims. These weren’t remotely truthful, not only because they relied upon statistical manipulation but because no one had a clue about BNT’s safety or efficacy. To this day, there are no clinical trial results.
The Clinical Trials That Don’t Exist
 An analysis of available positive RT-PCR tests and mortality results led the Oxford Centre for Evidence Based Medicine estimated a very tentative COVID 19 Case Fatality Rate (CFR) of around 1.4%. Based upon the figures reported to the FDA by Pfizer and BioNTech, this indicates a broad population based mortality risk from COVID 19 of 1.4(0.88/100) which is 0.012%.
An analysis of available positive RT-PCR tests and mortality results led the Oxford Centre for Evidence Based Medicine estimated a very tentative COVID 19 Case Fatality Rate (CFR) of around 1.4%. Based upon the figures reported to the FDA by Pfizer and BioNTech, this indicates a broad population based mortality risk from COVID 19 of 1.4(0.88/100) which is 0.012%.
Please bear this incredibly remote risk in mind as we discuss the early indication of the apparent threat to public health presented by the mRNA vaccine.
It is reasonable to work in terms of population risk because, while the chance of COVID 19 mortality seemingly increases with age, with the average age of death being 82 and a mortality distribution indistinguishable from standard mortality, the intention is to give the vaccine to everybody.
If we look at the “V-Safe Active Surveillance for COVID 19 Vaccines” reported by the U.S. Center For Disease Control (CDC), early indications of the recorded “Health Impact Events” (HIE) reveal a worrying level of adverse reactions from the mRNA vaccine. The CDC define an HIE as:
“Unable to perform normal daily activities, unable to work, required care from doctor or health care professional”
On December the 18th 112,807 people were injected with the Pfizer/BioNTech vaccine in the U.S. Of these, 3,150 were subsequently unable to perform normal daily activities, unable to work, required care from doctor or health care professional. This is an HIE rate of 2.8%.
This suggests that among the first 10 million people to receive the vaccine in the UK, around 280,000 may find themselves unable to perform normal daily activities, unable to work and require medical care as a result. As it is the most vulnerable who are the first to receive this vaccine, given the tiny risk of mortality from the COVID 19 disease, it is by no means clear that this is a risk worth taking.
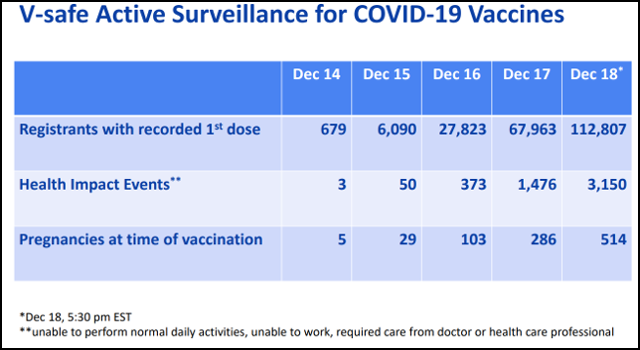
Not that any of the other vaccines seem any better. So far the CDC have noted more than 5,000 HIE’s for all vaccine being trialled on the population. Clearly, the potential exists that the vaccines will contribute to more deaths than the disease they allegedly protects vulnerable people against.
The Pfizer/BioNTech trial was registered as clinical trial number NCT04368728 with the CDC. Having recently discussed what I am about to share with you with people who simply refused to believe the evidence of their own eyes, I think it is important to stress that this is the Phase 3 Clinical Trial which Pfizer claimed they had concluded in their press release. There isn’t another one. This is it.
The CDC state:
“When available, study results information is included in the study record under the Study Results tab…….After study results information has been submitted to ClinicalTrials.gov, but before it is posted, the results tab in the study record is labeled “Results Submitted.”
 At the time of writing (21st December 2020) as can be seen by date of the archived ClinicalTrials.gov web-page, the Study Results tab reads “No Results Posted.” That is because there are no posted or submitted results from the Pfizer BioNTech trial of the BNT162b2 vaccine:
At the time of writing (21st December 2020) as can be seen by date of the archived ClinicalTrials.gov web-page, the Study Results tab reads “No Results Posted.” That is because there are no posted or submitted results from the Pfizer BioNTech trial of the BNT162b2 vaccine:
“No Study Results Posted on ClinicalTrials.gov for this Study”
Mainstream media reports, giving the impression that these vaccines have been found to be effective and safe are not evidence and they are not based on science. They are based on political policy and they report dangerous pseudo-scientific babble, masquerading as science journalism.
There will of course be mindless anti-rationalists who will call this dangerous antivaxxer nonsense. All the time insisting that it is perfectly safe to give a vaccine with a questionable safety profile, for which there are no completed clinical trials, to the most vulnerable people in our society. I am running out of patience with these people.
Vaccine Safety?
The start date for NCT04368728 was April 29th and the estimated trial completion date is January 27th 2023. The estimated end date of the primary or phase one of a three phase trial is June 13th 2021.
According to the “Current Primary Outcome Measures,” the minimum time frame for Pfizer to assess serious adverse events (SAE’s) is “6 months after last dose.” This is the minimum term for assessing SAE’s in phase one of the trial.
Phase one is the only part of the NCT04368728 trial to have been completed and published. It was published on the 14th October, 5 months and two weeks after the start date. Most of that period was taken up with recruitment an allocation. The minimum term for assessing SAE’s has not been met during Phase One.
During Phase One, 195 participants were split into 13 groups of 15 people. In each group 12 received one of two potential mRNA vaccine candidates (either BNT162b1 or BNT162b2) and 3 a placebo.
39 people aged between 18-55 and another 39 people aged between 65-85 received the BNT vaccine, now approved for global distribution. The threat of COVID 19, though tiny overall, is statistically zero for those aged 18-55. Those with any measurable risk from COVID 19 were in the older age group.
Of the 39 older people who received 2 doses of BNT about half of them experienced “fatigue,” roughly 15% had “chills” and 3 of them had a fever. The common side effects of BNT included nausea, headache (a very common BNT induced nervous system disorder) arthralgia and myalgia (very common), fatigue, chills and fever (again very common.) Other than fatigue, no one in the placebo group suffered these problems.
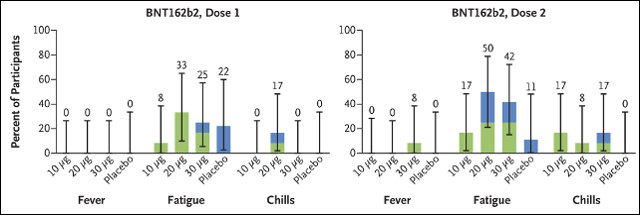
The study states, “Pfizer was responsible for the trial design; for the collection, analysis, and interpretation of the data; and for the writing of the report.” Therefore, it is reasonable to conclude that while Pfizer see the side effects of their vaccine as fatigue, chills and fever, the CDC refer to them as people who can’t work and need medical care.
The UK Medical and Healthcare products Regulatory Agency (MHRA) approved the BNT vaccine, to be given to vulnerable British people, based upon a study of 39 older people. This study reported a pretty high adverse reaction rate. It was produced exclusively from the R&D of the vaccine manufacturer. The MHRA questioned nothing.
They “approved” BNT in the certain knowledge that there were no completed clinical trials for this vaccine. In their Public Assessment Report they state:
“At the time of writing, the main clinical study is still on-going….It was concluded that BNT162b2 has been shown to be effective in the prevention of COVID-19. Furthermore, the side effects observed with use of this vaccine are considered to be similar to those seen with other vaccines. Therefore, the MHRA concluded that the benefits are greater than the risks.”
This conclusion and approval not only lacks supporting evidence it is utterly at odds with what little is known about BNT. While Pfizer and BioNTech only completed trials of the vaccine on 39 relevant test subjects, the results, even from this practically inconsequential effort, suggest the risk from the vaccine is greater than the risk presented by COVID 19. By a considerable margin.
This undoubtedly explains why the MHRA ordered software from European suppliers to deal with the slew of vaccine adverse reaction they presumably anticipate. They stated:
“The MHRA urgently seeks an Artificial Intelligence (AI) software tool to process the expected high volume of Covid-19 vaccine Adverse Drug Reaction (ADRs)….it is not possible to retrofit the MHRA’s legacy systems to handle the volume of ADRs that will be generated by a Covid-19 vaccine.”
From the way the manufacturers, politicians, regulators and the MSM have approached vaccine safety, it is clear that they collectively have at total disregard for the welfare of vulnerable people. We really must put aside this infantile notion that “the authorities” care about us or our loved ones. We mean nothing to them.
 COVID 19 is only an appreciable risk for the most vulnerable in society. It is a risk to the infirm elderly and people with existing life threatening conditions.
COVID 19 is only an appreciable risk for the most vulnerable in society. It is a risk to the infirm elderly and people with existing life threatening conditions.
If we look at the exclusion criteria for Phase One, these people were not in the cohort tested. Anyone with high blood pressure, asthma, diabetes or a high BMI were excluded from the alleged safety trial. But the vaccine is being given to the most vulnerable first.
Of the 39 older people at most risk in the phase one study, none of them had the serious comorbidities which the overwhelming majority of those who die “with” COVID 19 possess. The people actually at risk from COVID 19 nominally entered the BNT trials at phase 2 and 3. However, it appears every effort has been made to limit, if not completely remove, their number too. “Immunocompromised or individuals with known or suspected immunodeficiency,” were excluded.
Immunodeficiency is caused by a wide range of health conditions. Conditions such as undernutrition, polytrauma, stress after surgery, diabetes and cancer lead to immunideficiency. The people with the comorbidities associated with so called COVID 19 deaths were practically ruled out from the BNT vaccine trials.
NCT04368728 was designed as a 1,2,3 trial with all phases running concurrently. With regards to assessing safety Pfizer described systemic events as:
“Fever, fatigue, headache, chills, vomiting, diarrhea, new or worsened muscle pain, and new or worsened joint pain as self-reported on electronic diaries.”
The first 360 subjects randomised into the phase 2 and 3 trials underwent monitoring for systemic events for less than a week, following each dose:
“In the first 360 participants randomized into Phase 2/3, percentage of participants reporting systemic events [ Time Frame: For 7 days after dose 1 and dose 2 ]”
The same cohort of 360 test subjects were also monitored for Serious Adverse Events (SAE’s) for up to 6 months in phase 2 and 3:
“In the first 360 participants randomized into Phase 2/3, percentage of participants reporting serious adverse events [ Time Frame: From dose 1 through 6 months after the last dose]”
Pfizer also intend to report the percentage of all test subjects who suffer SAE’s:
“Percentage of participants in Phase 2/3 reporting adverse events [ Time Frame: From dose 1 through 6 month after the last dose ]”
But there are no reported results from either phase 2 or 3. No one has the faintest idea what the health risks of BNT are, especially for those it is supposedly designed to protect, and no one in authority gives a damn. Phase 2/3 clinical trials are now a moot point anyway.
The regulatory agencies have already approved the vaccine and health services have started injecting people with BNT. They do so after the manufacturers failed to properly test its safety on a 39 people who were in the at risk group but did not have the comorbidity that leads to claimed COVID 19 deaths.
The degree to which people have been misled into believing that these vaccines are known to be either safe or effective is almost beyond imagination. Sadly, we don’t need imagination. The evidence is clear.





Great article on the data on the tests. Keep up the good work eventually one or two more might get the message!
I just cannot get my head around the fact that tests have not established if it stops you getting seriously ill and secondly if it stops transmission and yet people think it’s the answer to the problem. When I point this out they just dismiss it and cannot compute the deception. I posted the following on Facebook on the 12 December, got a few likes and no criticism, also on a WhatsApp group. I give up
Here is the post
On the subject of the vaccines.
There are 3 things you need from them
1) to prevent the illness causing serious consequences, causing hospitalisation and death.
2) to prevent the transmission of the disease to others.
3) safe and to not cause other health issues. In the short term and the long term.
Strangely none the current crop of vaccines are testing the first 2 . If you think I making this up ( see BMJ article:- https://www.bmj.com/content/371/bmj.m4037). Unbelievable but true, Matt Hancock is lying to us, he says it will save lives without testing no1 that is simply untrue.
Without testing the transmission ,any arguments for compulsory vaccination are without any merit.
On number 3, too early to tell for long term. Secondly there are criticisms from a number of doctors about the health risks. However If I post the links to them they will be flagged as false information as Facebook are shutting down any alternative views on anything to do with vaccines. There will certainly be some adverse reactions but the scale of which is unknown at this moment.
The MHRA who have authorised the use of the phizer jab are one of the most corrupt organisations. There is a litany of outrageous behaviour over the last 20 years, including falsifying 6000 test data to allow them to authorise the use of a cervarix HPV vaccine. They are essentially an arm of Big Pharma, dressed up as a regulatory body.
Why would anyone who was informed would allow this to be injected into themselves is beyond me. It strikes me as act of Blind faith in Pfizer, whose track record is hardly one anyone would be proud of.
Excellent stuff David. Likewise. Keep up telling the truth. What else can we do?
Hello again Iain and thank you again for something extremely important and very much close to me. First I’d like to agree with David’s response above in all he says. I’m a British woman over 70. I was somehow persuaded by the BBC and the voice of MHRA Chief Executive Dr June Raine saying that the Pfizer vaccine had been tested on thousands of people. I am sure I heard her say this. But I cannot find a tape anywhere of it now! Rather like a quotation I gave of Bill Gates that I knew he said and had replayed a few times, but when I returned to the recording it had been altered. I would not have forgotten hearing her say there had been thousands of subjects. I’m a retired Research Fellow, so did research myself therefore I’m not uninitiated. She says they are doing a” rolling review” and starting the next stage before finishing the one before… She is an appalling speaker – reading her notes so badly which makes it hard to follow e.g. see https://youtu.be/kEcPOXa76j8. But now I find her talking to us as though we are 5 years old saying how carefully they read the Pfizer report and had other independent bodies watching over. She appears to be saying that they were doing the research not Pfizer! It all sounds very muddled. You can tell that the Questioners are only allowed to couch their questions in a certain – very supportive – style too. When I listen I just know she is covering herself and doesn’t understand research anyway. But on https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19-vaccination-advice-from-the-jcvi-2-december-2020/priority-groups-for-coronavirus-covid-19-vaccination-advice-from-the-jcvi-2-december-2020 the Government say their “advice has been developed based on:….Phase 1, 2 and 3 data on the Pfizer/BioNTech mRNA vaccine and …” this “Updated 3 December 2020”. Also Chris Whitty the Chf. Med. Officer seems to say on another tape they are still gathering phase two data, or he fluffs over saying how cleverly they collect data.. It sounds extremely fishy to me. There was a time when a Jeremy Paxman kind of Questioner would want to know what the hell was actually happening and how much was Pfizer making to kill off the Grannies more quickly than ‘covid’ itself?
I have just learned too that people with shellfish allergies should not take the Pfizer vaccine! Well, apart from having severe reactions to vaccines twice as a very small child I also am allergic to shellfish… But I have a Doctor who is quite forceful. I do feel threatened here in middle of England, on my own not wanting this.
Your work is so vitally important at this time. Thank you Iain.
Thanks Leslie. Thanks to your excellent comment I have updated the post. They have essentially conflated phase 1 data (based upon an tiny cohort study) with phase 2 and 3 data which is nowhere near publication. They have then claimed that phase 1 data is the same as phase 2 and 3 data (which it isn’t) applied relative instead of absolute risk from phase q data to make up impressive efficacy claims and have not even bothered completing phase 1 safety assessments before making their claims about the vaccines. It truly beggars belief.
Thanks Ian, I too am aghast at what they are allowed to get away with. In their original article, ‘Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine’ they say under ‘quick take’ “Collection of phase 2/3 data on vaccine immunogenicity and the durability of the immune response to immunization is ongoing, and those data are not reported here.”
I feel like putting it large; “THOSE DATA ARE NOT REPORTED HERE”. Yet they write a paper and the MRHA then say they have looked at the data very carefully and decided we shall go ahead with the ‘vaccine’ and stick this concoction into everybody beginning with the oldest people first…..
By the way, I was once the Research Psychologist on a large International Research project into a Molecular Genetic Study. Everybody else was either a Paediatrician or Psychiatrist. Doctors do not know how to do research. Not unless they are very unusual. I had to teach them starting from the very basic concepts. They were very nice about it as Psychiatrists and Paediatricians are usually lovely (also Neurologists I found). I think our Dr Raine in charge of the MRHA knows nothing about research.
I’m feeling pretty despondent these days but you do give me hope Iain. To have an honest person who is intelligent and prepared to speak out in truth does give me hope. Thank you.
Thanks Leslie. And comment like your give me hope too. It can feels sometime like you are screaming in the wind so I cannot express to you how important feedback from interested readers is to me. Especially when they provide more valuable insights as you always do. Thanks Lesley.
Thanks, Iain.
That was very informative.
Especially the point that the population at large are now the clinical trial for phase 2 and 3.
This is a politcal/social/economic disease. It is psyops probably years in the making. We say therefore it is.
We all suffer from confirmation bias. But when the information and facts are laid as bare faced as they are, I wonder what sort of group think entices healthy people to take a PCR test or allow themselves to be injected with heaven knows what.
I see no end to this clusterfuck.
Thanks Graeme. There certainly wont be any end to it of we give up. Keep going mate.
Very good review!
However there is one glaring omission. My relatives in the US are scared into taking the vax because they say they are reading that 30% of those who recover from ‘covid’ have significant complications months later. What of this claim, anyone?
Thanks Ed. I haven’t really looked into so called “long COVID.” However my initial observation is that all viruses that are capable of making us ill can have lasting effects. There is so much fear-mongering disinformation surrounding COVID 19 that I would not be surprised if this risk were no more pronounced for COVID 19 than for any other respiratory virus.
Great article, Iain. I’ve urged my wife to read it, as she says she wants to get the genetic modification done (I refuse to refer to it by the name given to it by the media).
I think the biggest issue with this experiment is that people are being given the impression that life will go back to how it was before the phoney coroney once they get jabbed, but that simply isn’t going to happen. The experiment won’t immunise you from the made up disease, so masks still apply, it won’t stop you spreading the made up disease, so physical distancing still applies and in a few weeks, months or whenever, the next new phoney variant will pop its head up and we’ll all be placed in lockdown again. This can be done repeatedly and indefinitely until all the pieces are in place for whatever it is they have planned for us.
Keep up the good work.
PS spelling Nazi head on for a minute. In the article you’ve spelt spinal cord with an h. (you can delete this bit of my comment!)
Thanks Simon. I agree taking the vaccine won’t change anything but they will blame no change on people’s “bad behaviour.” Thanks for pointing out errors, I am a one man band and don’t have an editor so I am grateful. Please don’t worry about pointing out errors. I need to know.
Wondering please if the in-this-together.com would consider having an option of downloading a printable version of this article. Just as would like to share with friends and family yet feel they’d be more likely to read it received from me in the mail as a document.
thanks Mazza but I’m afraid I don’t know how to add that option but I will look into it.
In the meantime please note I use a Creative Commons License at ITT. All content is free to download, share, print and distribute as you see fit. All I ask is that any changes made are clearly marked and appropriate accreditation given.
You can cut and paste the content into an Open or Libre Office text document and then export this as a pdf for printing if you like.
Hello Thank you for all your good work. Its really impressive. I also made a film about the relative risk v absolute risk.. Its here https://www.youtube.com/watch?v=SpVczBygQtI&t=80s mixed in with a few other things.
The paper I quoted regards relative risk “it should never be used alone” related to informed consent is here https://pubmed.ncbi.nlm.nih.gov/31345957/ I hope it is useful.
My investigative work is nowhere near as thorough as yours. I tend to jump around a lot – as you’ll see from the vid. However, we are all doing our best. You can hear Im cross as I read . Sorry about that. It just gets to me sometimes.
Many thanks for all you are re doing Beki. Your video is very good. We just need to keep the putting the info out.
Hi Iain. As this genetic manipulation is only authorised for emergency use, do they have to keep us in lockdown to keep their state of emergency? until they’ve shot us all up?
Several pregnant nurses have lost their babies after being shot.
https://childrenshealthdefense.org/webinar/the-covid-vaccine-on-trial-if-you-only-knew/
https://dailyexpose.co.uk/2021/02/08/official-data-on-adverse-reactions-to-vaccines/
There is a cunning ploy here. They haven’t declared an emergency. Had they done so they would have had to use the 2004 Civil Contingencies Act https://www.legislation.gov.uk/ukpga/2004/36/section/1
However there are limitation on what the government can do under that Act – https://www.legislation.gov.uk/ukpga/2004/36/section/23
So they didn’t invoke it in order to create what was effectively an Enabling Act with the Coronavirus Act. This has given them practically unlimited power because they can just trot out secondary legislation (secondary instruments) without any Parliamentary scrutiny. So they can do anything they like in effect.
Hi Iain,
Do you know of a pro-forma Informed Consent check list for these drugs?
Such a document would cover :
What mRNA is.
How it works.
History of approval 🙂
Trials as you have outlined above.
Absolute risk (Hard for average person to understand. Most Doctors don’t even understand Bayes)
etc…
My thinking. Hand the Doctor (not nurse) the form. have them fill it in and then sign off that they recommend that you are given the drug and accept total liability for damages. or not, as the case may be.
Hi Graeme, I have seen a few suggested templates online and yes, if we are ever forced to take a drug against our will, a suitable informed consent that acts as a notice if individual liability will be necessary. Unfortunately I can’t remember where I’ve seen them. Sorry.
They can “vaccinate” me while performing preparations for my autopsy.
Yep. My body my choice. I see no need to explain it any more than that when they come knocking.
Hi Iain, Thanks for your dedicated work, can you please supply a data reference for this point :
>> based upon a study of 39 older people.
Thanks in anticipation
Colin Quinsey
Thanks Colin. That is wrong, it’s not 39 it’s 36. I don’t know what got into my head there. But seeing as it’s less, I’ll leave it as it is.
I’ve linked to the archived paper which doesn’t show Figure 1 so well. Go to the original here: – https://www.nejm.org/doi/full/10.1056/NEJMoa2027906
Then check out Figure 1 and you will see that a total of 36 (not 39) people aged between 65 – 85 received BNT162b2 (which was the one approved.)
Sorry about that.
Since this article was published we have had more than 3 months experience of the vaccine. How about an update? Do you agree that all the evidence suggests that the net benefits of vaccination, in terms of lives saved from COVID deaths (check the statistics in any country with a large vaccination program), exceed by far the exceedingly small number of deaths resulting from vaccination (I don’t doubt there are a few)?
Thanks Ian. I will soon be creating a flood of content at Iain Davis. I have been working on a big project but am still writing for the UK Column and others. I am not aware of any net benefits from vaccination so far. I am aware of the claims made that the reduction in mortality among vulnerable groups is a consequence of vaccination. However, It seems equally plausible to me that it is actually a consequence of the change in seasons.
The vaccine roll out not only coincided with a significant increase in care home mortality it was well timed to take advantage of the normal end of the winter respiratory season. I think, in order for there to be any evidence of a notable net benefit from vaccines, we need to wait for the return of the respiratory illness in the Autumn. Presumably, if there is a net benefit as you suggest, this will clearly be evident at this time as COVID 19 mortality should be significantly lower among the most vulnerable vaccinated groups.
I also accept that the 600 or so deaths apparently caused by the vaccines in the UK so far (according to the MHRA) is a relatively low figure compared to COVID 19 mortality. However not only do I think COVID 19 mortality has been massively overestimated. I believe the true COVID 19 mortality figure in the UK is somewhere in the region of 15,000 – 18,000. You can read my reasoning here if you are interested: https://www.ukcolumn.org/article/deceptive-construction-why-we-must-question-covid-19-mortality-statistics
I also think it likely that vaccine ADR’s have been significantly under reported. Certainly there is plenty of anecdotal evidence that this may be the case. I intend to research this possibility further but do not know at this stage if their is any validity to these claims.
I fully accept that correlation does not prove causation and I am not denying that there may be a net benefit from vaccination. I would be pleased to look at any evidence you can provide to back up that notion.
Is there really a “Covid mortality rate”? What would it mean – death from Covid only? The death data has been corrupted because covid deaths are determined by positive test result which is insanity. Surely, the only reliable way of looking at deaths is the overall annual mortality rate. I could not see anything significant in the 2020 mortality rate to suggest there was a pandemic. It was the 12th lowest death rate on record. Since it is mainly the elderly who are dying and they have comorbidities, then covid is only one factor in their death and perhaps not the most important. Deaths rates must go up eventually when we have several years of reducing death rates as in the UK.
Good question. The data is relatively robust but the inputs are virtually meaningless. Calling tests “cases” and so forth. You are right 2020 was only the 9th highest mortality rate in the first two decades of the 20th Century. Even with all the fake statistical inputs (calling Flu COVID for example) there is still no evidence to support the notion of a “global pandemic.” At least from a UK statistical viewpoint. If you look at the distribution of mortality, which you would expect a global pandemic to alter, there is nothing. As you rightly highlight the average age of a COVID death in the UK was 82. Which is the same as the average age of death in any other year. More telling was the distribution of mortality across the age ranges. This too was identical to normal distribution. No evidence of a pandemic.
Target organs of SARS-CoV- 2 mRNA Vaccine
See Japanese study. N.B.* The ‘Pharmacokinetics: Organ Distribution’ tables are in English:
https://www.pmda.go.jp/drugs/2021/P20210212001/672212000_30300AMX00231_I100_1.pdf
I have only just found this, but more relevant than ever with the passage of time. Fortunately, I had to investigate RCTs in relation to a complaint about an operation, so I found out all the trick that are used.
An issue that concerns me about the trials is that we were told that mask wearing, social distancing and lockdowns all reduced the risk of infection and spread. The vaccine trials were conducted while these other measures were in place and if the assumptions about their benefits are true then they could influence the results of the vaccine trials. The trials must be designed to eliminate all other factors which might influence the results and if they cannot be eliminate they have to be taken into account in the risk calculations, reducing the benefit of the vaccination.
I also suspect that there is no effective placebo group because some have been vaccinated and others may have acquired natural immunity.