
In my previous article I committed the journalistic sin of predicting the future. I anticipated that the BBC’s proposed documentary, “Unvaccinated with Professor Hannah Fry,” would be little more than propaganda.
The BBC said it would place seven ordinary unvaccinated citizens in a house and then try to convince them that everything they thought they knew about the jabs was based upon mis/disinformation. The BBC claimed it wanted to provide viewers with an “eye-opening investigation” that would “fully explore this complex and deeply divisive debate.”
While the press release for the program promised a “documentary,” I ventured that the BBC would actually manipulate the reported data, cherry-pick the science, omit vital information and produce, in effect, a sales pitch for the COVID-19 jabs. So it is, I admit, with a degree of schadenfreude that I can now say this is precisely what the BBC did.

In my aforementioned article, I incorrectly interpreted the UK Health Security Agency’s (UKHSA’s) stated 70.2% total vaccine coverage figure as a mean and not the median that it was. Consequently, my estimation of 11M unvaccinated UK adults was wrong.
Nonetheless, as expected, the BBC opened its program with a statement that misreported the statistics. It claimed there were just 4M unvaccinated UK adults. For a multi-billion-pound media operation like the BBC to repeatedly report the vaccination statistics incorrectly and consistently underreport unvaccinated numbers is not just an inadvertent error. It is a deliberate fabrication of the facts.
According to the Office For National Statistics (ONS) in mid-2020 the adult population of England (over 18) stood at just under 46M. Given population growth, we can safely use a figure of at least 46M adults in England in 2022.
UKHSA reports that approximately 44.5M people in England have received at least one dose of a vaccine. Approximately 3M of them are under 18. Thus, we can say that at least 4.5M adults in England, or around 9.7% of the English population, have not received a single dose of the vaccine. England accounts for about 84% of the UK population. Assuming almost identical vaccine coverage elsewhere in the UK, this suggests that approximately 5.3M UK adults have not received a single dose of the vaccine.
The UK government‘s definition of “vaccinated” is “2 doses of an approved vaccination, or 1 dose of the Janssen vaccine.”
The Janssen vaccine is the only single-shot vaccine approved in the UK, and use of it is rare. To be considered “vaccinated,” two doses of the Pfizer or AstraZeneca or Moderna jab are required. Therefore, UKHSA data indicates that there are approximately 40M “vaccinated” adults in England. This means that there are around 7.2M unvaccinated adults in the UK, representing approximately 13.5% of the UK adult population.
As we can see, Fry’s opening statement that “there are still around 4M adults in the UK who remain unvaccinated” was flagrantly false.
After making that misleading remark, Prof. Fry questioned the rationale for remaining unvaccinated:
I want to understand why and find out if anything can change their [the participants’] minds.
From the start of the BBC’s program, it was clear that the filmmakers had an agenda: convince everyone to take the vaccines.
In short, the purpose of the program was not to explore the debate, as claimed in the BBC press release, but rather to persuade people to get the jab as well as maintain belief in the COVID-19 vaccine among those who are already jabbed.
The BBC never had any intention of objectively reporting the facts or encouraging any genuine discussion of the evidence. Its purpose, as usual, was to promote the government narrative. This was exemplified by Prof. Fry at the start of the program’s penultimate segment when she said:
I just want to remind everyone just how critical the vaccines have been in allowing us all to go back to normal.
Back to normal? The policy response to this alleged pandemic has so changed the public’s relationship with the government that it can no longer be considered “normal.” The removal of our freedoms and official denial of the existence of our natural rights has convinced most people to adapt to a new model of government. The illusory “social contract,” neither seen nor signed by anyone, now demands total acquiescence to this “new normal.”
Some might think that the UK government’s reaction to the alleged existential threat was wise. Others will argue that government abuse of our inalienable rights is never justified under any circumstances. The point is that these are policy decisions, not the inescapable consequences of a so-called pandemic.
Recently UK junior health minister Syed Kamall said:
If hospitalisations start affecting the NHS backlog then clearly measures may well have to be introduced[.] [. . .] If that gets out of control then of course we will stand up the measures that we have previously.

Kamall blithely announced that, if it’s deemed necessary, the government will once again restrict our freedoms and ignore our rights. It might order us to stay at home (lockdown), deny our freedom of movement, ban us from gathering, decree whom we can meet, compel us to wear masks and demand that we prove our health status before we are “allowed” to participate in society.
Prior to the alleged COVID-19 pandemic, no way would the UK public have tolerated such a dictatorial proclamation from any politician. But now statements like Kamall’s receive barely a murmur of dissent. The vast majority of the population meekly accepts that the government requires these draconian powers to impose its authoritarian will upon us whenever it claims there is good reason.
As a society we have been transformed to accept dictatorship without question. Irrespective of their impact upon public health, the jabs are part of the biosecurity controls that take precedence over everything and everyone whenever the government wishes to change our behaviour.
To sum up, the COVID-19 jabs most assuredly have not enabled us to return to any kind of recognisable “normal.” Fry’s claim was absurd. Indeed, “Unvaccinated with Professor Hannah Fry” could have more accurately been titled “Propaganda with Professor Hannah Fry.” So let’s take a closer look at the BBC’s propaganda.
The Denial of Adverse Events
A participant named Nazarin was filmed telling Prof. Fry about her friend who started having neurological problems five days after the Pfizer jab and subsequently suffered a stroke and multiple heart attacks. Fry asked Nazarin:
How can you be sure that was the vaccine, and not something that would have happened anyway?
Nazarin’s reply was pertinent:
If you’ve been completely healthy before, that one thing changed and then days later you’re suddenly experiencing all these things you have never had before, like paralysis and seizures, the chance of that happening to someone so young. I would say, not possible. [. . .] It’s not just her, there are so many people going through the same thing.
Fry’s response to Nazarin sounded reasonable. Referring to the percentage chance that a healthy young person’s severe health event soon after vaccination may not be attributable to the vaccine, Fry said:
It’s not zero, though. . . .
True enough. But what Fry did not concede, as highlighted by Nazarin, is that it was likely that the adverse event (AE) was caused by the jab, given the circumstances. Prof. Fry then added:
I just don’t think it’s enough to say it’s happening a lot, without the evidence for it.
Nazarin and fellow participant Vicki later gave an interview to GB News in which they revealed that the BBC excluded key witness accounts from the program. For example, Nazarin said she repeatedly told the BBC that her great-grandmother died shortly after receiving the jab and that her grandmother had a stroke following her jab.
Vicki reported that Nazarin wasn’t the only participant among the seven to have told the BBC about family members who had possibly suffered a severe adverse event as a result of the jab. None of these personal accounts were reported by the BBC.
Prof. Fry’s insistence upon evidence would have been reasonable only if the BBC had been willing to consider—and, perhaps more importantly, objectively report—all the evidence. But the BBC did not do that.
Prof. Fry invited the seven unvaccinated participants to discuss vaccine adverse events. Yet at no point throughout the whole program did Fry actually report what the numbers of reported AEs were. Instead, she was eager to repeatedly suggest that there wasn’t really any link between reported AEs and the vaccines.
For instance, she cited a paper on the nocebo effect, which found that people sometime experience AEs as a psychosomatic reaction. Fry told the participants that 76% of claimed AEs “from the vaccine” could be attributed to this psychological quirk:
There was one study in America, the overall result of that study was that 76% of common adverse effects from the vaccine were essentially down to the expectation that you would feel rubbish after the vaccine.
The professor’s statement was highly misleading. What she said was not what the findings in the paper indicated.
The paper was a meta-analysis (combining data from a number of studies) which looked at the systemic (common) AE statistics for two groups of almost equal size. One cohort of 22,578 people received an “inert placebo.” The jab recipient group was a similarly sized 22,802. The paper stated:
Systemic AEs were experienced by 35% of placebo recipients after the first dose and 32% after the second. Significantly more AEs were reported in the vaccine groups, but AEs in placebo arms (“nocebo responses”) accounted for 76% of systemic AEs after the first COVID-19 vaccine dose and 52% after the second dose. [. . .] [T]here were proportionally more moderate and severe AEs in the vaccine groups after the second dose.
This means that 76% of all systemic AEs across both cohorts—vaccinated and unvaccinated—were reported in the placebo (unvaccinated) arm. It in no way implies that 76% (or 52%) of the reported systemic AEs in the vaccinated cohort were attributable to the nocebo effect, as Fry tried to assert.
The paper graded AEs from 1 to 4 as follows: 1(mild), 2 (moderate), 3 (severe), 4 (life-threatening). A “systemic” AE (grades 1 and 2) is a mild adverse reaction, such as temporary swelling, brief headache or nausea. A “severe” AE (grades 3 and 4) is an adverse event that may “jeopardize the patient and may require medical or surgical intervention,” according to the US Food and Drug Administration (FDA). Severe reactions include breathing problems, blood disorders, seizures, disability or permanent damage, hospitalisation, a threat to life and death. The BBC did not make this distinction clear.
Again, note that both cohorts—vaccinated and unvaccinated—in the cited study were of roughly equal size.
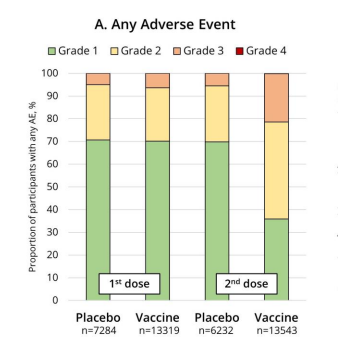
Let’s look at the placebo group. Following the first dose, out of the 7,284 claimed AEs, about 5% were allegedly severe, which equates to some 364 severe AEs in total. Following the second dose, there were roughly 312 severe AEs. Given that the people in the placebo group received an inert substance, it’s likely that a high proportion of their severe AEs were attributable to the nocebo effect.
Now the vaccinated cohort. The first dose produced 13,319 reported AEs, of which approximately 7%—or about 932—were severe. If we account for the likely nocebo effect, this suggests that around 570 of these severe AEs were potentially attributable to jabs. After the second dose there were 13,543 total AEs recorded. Approximately 22% of them were severe. Subtracting the likely nocebo numbers, this implies that, out of the vaccinated cohort of 22,802, there were more than 2,600 severe AEs possibly associated with the second jab.
The paper’s findings indicate that approximately 11% of second dose COVID-19 jabs reportedly resulted in a severe adverse event. The BBC and Prof. Fry did not wish to report this.
Prof. Fry misrepresented the paper’s finding in an attempt to convince both the participants and the BBC audience that more than three-quarters of reported AEs are probably attributable to the nocebo effect. Not only was this deceptive, but Fry failed to report the deeply concerning results that were reported in the paper with respect to severe AEs.
Later, Prof. Fry admitted that anaphylaxis and myocarditis are linked to the Pfizer jab. She also acknowledged that blood clots are associated with the AstraZeneca jab and that Bell’s Palsy (BP) and Guillain-Barre Syndrome (GBS) have also been flagged as potential “rare side effects.”
Prof. Fry illustrated one of her claims with jelly beans. Knowing that myocarditis—inflammation of the heart muscle—is the most commonly reported severe AE attributed to the COVID-19 vaccines, she claimed that only one of 33,000 jelly beans represented the alleged vaccine-induced case rate of myocarditis. However, as we shall see, there was no basis for her to claim such a low relative risk.
The professor isn’t the only one to grossly underestimate the relationship between the jab and myocarditis. The UK Medicines and Healthcare Products Regulatory Agency (MHRA) has collated the Yellow Card surveillance reports, which suggest there may be 1,112 myocarditis AEs associated with the COVID-19 jabs in the UK. The MHRA calls such an event a possible adverse drug reaction (ADR).
It’s important to note that in 2018 the MHRA estimated that only 10% of severe ADRs are reported to the Yellow Card system. Since then, the MHRA has done nothing to remedy the problem of an underreporting rate as high as 90%. Indeed, there could be more than 11,000 myocarditis ADRs associated with the COVID-19 jabs, for all we know.
In 2021 the MHRA updated its 2018 data with this caveat:
These estimates [of 10% of severe ADRs] should not be used as indicators of the reporting rate for COVID-19 vaccines, for which there is high public awareness of the Yellow Card scheme and the reporting of suspected reactions.
Perhaps so, but the MHRA hasn’t produced any estimates for COVID-19 vaccine ADR reporting rates. To what extent has “public awareness of the Yellow Card scheme” increased reporting rates, if at all?
Could reporting rates be up 50%? Or 20%? Or as little as 0.4%? How likely is it that doctors, who also submit Yellow Cards, correctly associate an adverse event with a vaccine? We have no idea. Nor, it seems, do the MHRA or Prof. Fry or the BBC.
The MHRA stresses that a reported ADR may or may not be caused by a jab. It has established a data analysis method that theoretically enables the MHRA to identify concerning signals in the data:
We apply statistical techniques that can tell us if we are seeing more events than we would expect to see, based on what is known about background rates of illness in the absence of vaccination. [. . .] [W]e generally do not expect all suspected side effects to be reported on Yellow Cards.
For example, the MHRA contrasts the reported Yellow Card incidents of myocarditis to the background rate of the same disease. It then applies comparative statistical analysis to identify what it and Prof. Fry call a “rare” ADR associated with the jabs.
As frequently noted by the MHRA and as mentioned above, the Yellow Cards are only capturing a small proportion of the ADRs. The only question is, what proportion?
All we have from the MHRA is a published estimate that the Yellow Card reporting rate could be as low as 10%. Consequently, the possibility exists that 90% of potential ADRs are not captured by the reporting system. Presumably, the remaining unreported ADRs could then erroneously contribute to the observed background rate for that condition.
This skewed data then forms the inputs for the MHRA’s statistical analysis. The MHRA may be significantly underestimating the possible ADRs while wildly overestimating the comparative background rate. There is no evidence that it has done anything about this problem, and there is a strong possibility that its so-called “analysis” is complete junk.
In regard to the monitoring of myocarditis, the MHRA claims:
There has been a consistent pattern of higher reporting of these suspected events with the COVID-19 Vaccine Pfizer/BioNTech and COVID-19 Vaccine Moderna. [. . .] These reports are very rare[.]
Without fixing the underreporting problem, there is no reliable evidence to support the MHRA’s claim that these possible ADRs are “very rare.” On the contrary, the scientific evidence suggests reason for marked concern.
US and Israeli researchers found that the overall incident rates of myocarditis among those who received the Pfizer jab has more than doubled. Myocarditis impacts some demographic groups more than others. For people aged 18–24, particularly but not exclusively males, French scientists found that the rate increase following the Pfizer jab was more than eight times higher and following the Moderna jab a staggering thirty times higher.
For Prof. Fry to dismiss, by omission, these legitimate concerns using a spurious, statistically inaccurate jelly bean analogy is, frankly, appalling.
Throughout the program, Prof. Fry and the BBC persistently relied upon statistical claims that are officially acknowledged to be inaccurate. At no point did the BBC disclose this to its audience.
For example, Prof. Fry addressed an information leaflet produced by people who are concerned about vaccine safety. The document, titled “Consent Checklist,” urges would-be jab recipients to consider some key information before they opt to get the jab.
The document reminds people that the manufacturers have no civil liability for any harm caused by their products, that the jabs don’t protect against infection or stop transmission of SARS-CoV-2, that AEs associated with the jabs are potentially serious and that, due to the lack of clinical trials, the long-term health impacts of the jabs are unknown. All of which is true.
In its unflinching investigation of the debate, the BBC didn’t bother to reveal any of the points made by the “Consent Checklist.” Instead, Prof. Fry called it “anti-vax propaganda.” She was apparently irked because the document stated that there was a calculated 1:29,389 chance of dying from a jab. She said:
It’s my job to look into numbers like this and I can tell you, as an absolute fact, this is complete nonsense.
How does Prof. Fry know this? She didn’t explain. She provided no sources. She simply threw out a claim without evidence. Perhaps we should trust her simply because she works for the BBC and says she’s an expert?
We can be certain that people have been killed by the jabs. Sadly, this includes one of the BBC’s own, Lisa Shaw. And there have been other proven deaths from the COVID-19 jabs. As of January 2022, the ONS has reported 15 UK deaths clinically coded as being caused by a COVID-19 jab.
As pointed out by Professor Lawrence Young, a virologist based at Warwick University, the official coding of a vaccine death alone is unlikely to reflect the totality. Given the data from the MHRA, he noted that the ONS figure was too low.
Prof. Young said that there was a need “for more detailed investigation to reconcile these different estimates.” He added that to make this assessment a “detailed review of death certificates, autopsy (if available) and medical records” would be needed.

Herein lies the problem with any claims made about UK mortality caused by the jabs, including Prof. Fry’s. The MHRA has done nothing to investigate any of the reported vaccine-related deaths. It is content simply to continue to search for “signals” within officially recorded figures which, by its own admission, are wrong.
Consequently, all anyone can say is that the MHRA has recorded 2,207 possible vaccine-related deaths in the UK, which could equate to more than 22,000, given the estimate of 10% reporting. We also know from UKHSA that approximately 48M UK adults have been jabbed.
If we ignore the acknowledged underreporting problem, this currently suggests a possible 1:22,000 risk of death caused by vaccination. If we account for the possible scale of underreporting, though, the current jab-related mortality risk is potentially 1:2,200.
These calculations do not prove the mortality risk associated with the COVID-19 jabs; they merely suggest it. This was made clear in the document that Fry attacked for the cameras.
That document stated that the estimate of a 1:29,389 risk was based upon “officially reported” figures. It was an accurate estimate given the available evidence at the time. As the reported risk did not reflect the known Yellow Card underreporting issue, the quoted 1:29K risk was, in all probability, the lowest possible estimate.
As highlighted by Prof. Young, without a thorough investigation we don’t know what the truth is. Absent further analysis, there is no reliable evidence to inform any assessment of the relative risks associated with the jabs.
So how Prof. Fry could be “absolutely certain” that the claims made about vaccine mortality rates were “complete nonsense” is mystifying. Despite her conviction and self-declared expert status, it was actually Prof. Fry’s seemingly authoritative assertion that was complete nonsense.
What Prof. Fry asserted was entirely in keeping with the BBC’s propaganda message.
During the documentary, the BBC downplayed and denied any adverse events associated with the COVID-19 vaccines wherever possible. It deliberately misinterpreted the available statistical evidence, omitted or misreported the science that ran contrary to its agenda and attempted to thoroughly deceive the participants and its viewers to encourage them to get potentially harmful jabs.
Obfuscating Concerns About The Trials
Prof. Fry held a discussion with two participants, Nazarin and Vicki, who asked her to clarify the vaccine’s approval and trial status. Fry and the BBC gave an entirely false impression that “approval” signifies that the jabs have completed clinical trials.
For instance, Prof. Fry stated that the jabs had been through the same approval process as paracetamol. This was not true.
The Access Consortium of regulatory authorities from the UK, Canada, Australia, Switzerland and Singapore explain why this is not the case:
Initial vaccine approvals or emergency authorisations may be based on interim analyses of ongoing randomised placebo-controlled phase 3 clinical trials.
Phase III trials do not need to be complete for a COVID-19 jab to be “approved.” They remain incomplete for the original Pfizer and Moderna jabs to this day.
There is a distinction between “approval,” under emergency authorisation, and the “marketing authorisation” of a medication for distribution to the public. Or at least there used to be.
The Pfizer Comirnaty jab, for example, has yet to meet the required standard for full marketing authorisation. To get around this problem, in 2021 the MHRA and the EU regulator (the EMA) created something called Conditional Marketing Authorisation (CMA).
Explaining CMAs, the MHRA stated:
The MHRA may grant a CMA where comprehensive clinical data is not yet complete, but it is judged that such data will become available soon.
In other words, this new licensing workaround enables the jabs to receive so-called “marketing authorisation” without the burdensome necessity of completing any Phase III clinical trials. That is precisely the current condition under which the MHRA gave Conditional Marketing Authorisation to Pfizer’s Comirnaty jab.
Though Pfizer hasn’t completed any trials or posted any trial results, it might in the future. That’s good enough for CMA, as far as the MHRA is concerned. The MHRA has based its licensing of Pfizer’s drug upon whatever Pfizer has chosen to report.
The BBC, represented by Prof. Fry, reported none of this crucial context. Instead of honestly answering the participants’ questions, the BBC elected to thoroughly obfuscate the issue and redirected viewers attention toward out-and-out falsehoods via a series of highly misleading statements by Fry.
Responding the Vicki’s legitimate question about the status of the trials, Prof. Fry concluded by saying:
Vicki is right in some ways. The vaccines do indeed go on to Phase IV trials after approval. But this is normal. Phase IV trials are the ongoing surveillance of the drug after rollout.
 While it is “normal” for jabs to go into Phase IV trials, it is also “normal” for drugs to complete Phase III trials before they are rolled out. The latter has not happened with respect to the COVID-19 jabs—but Fry forgot to mention that minor detail. Vicki was right in more ways than Prof. Fry cared to admit.
While it is “normal” for jabs to go into Phase IV trials, it is also “normal” for drugs to complete Phase III trials before they are rolled out. The latter has not happened with respect to the COVID-19 jabs—but Fry forgot to mention that minor detail. Vicki was right in more ways than Prof. Fry cared to admit.
This lack of any genuine regulatory oversight has also become “normal.” The MHRA no longer considers itself a safety monitoring regulator of pharmaceutical products.
Speaking at the MHRA Board meeting on the 24th of March 2022, the chief executive of the MHRA, June Raine, said that the MHRA is “an enabling regulator, no longer a watchdog.” She added that its role is to accelerate “access to innovative products.”
This is in line with the UK government’s commitment to the G7’s 100 Day Mission (100DM). This is a global public-private partnership initiative to develop a so-called “armamentarium” of diagnostics, therapeutics and vaccines (DTVs).
The extremely dangerous idea is that modern DTVs, largely built upon mRNA platform technologies, don’t really need any extensive trials or safety surveillance. As soon as a global public health emergency is declared by the World Health Organisation (WHO), it will trigger governments around the world to feed taxpayer money to pharmaceutical corporations—government “partners”—who will get the DTVs on the market within 100 days.
As far back as March 2021, the MHRA was preparing to move away from acting as a public health “watchdog” and toward “enabling” pharmaceutical corporations to release their products as quickly as possible with the minimum amount of fuss. In reference to what were being called “tweaked” vaccines—namely, new iterations of existing jabs designed to tackle allegedly novel variants of COVID-19—the MHRA announced:
Regulatory Authorities do not consider an updated coronavirus vaccine to be an entirely novel product with the resulting requirement for lengthy full-blown clinical studies. [. . .] Evidence gathered by the large pivotal clinical studies for initial authorisation and by mass vaccination campaigns is a strong foundation for this approach. [. . .] From a clinical perspective, clinical efficacy studies prior to approval are not required.
Leaving aside the fact that the “evidence gathered by the large pivotal clinical studies” came from trials for which “no results have been posted,” the MHRA claimed that the mere act of it “approving” a COVID-19 jab somehow constituted a “strong foundation” for it not needing to bother reviewing any future clinical trial data before “approving” the next drug. Frankly, there is no reason to imagine that the MHRA is even interested in public health.
Yet the BBC’s expert, Professor Hannah Fry, in response to Vicki and Nazarin, said:
There are different versions of the vaccine. It is possible for one version to be approved while simultaneously companies and the researchers are running clinical trials for subsequent versions. So those two things are not in conflict with one another. So every time you get an adaptation to the vaccine, you have to go back through the whole process and demonstrate, not just that it works, but that it is safe.
The “whole process” is nothing like the one described by Fry. “Approval” is not based upon clinical trial results, as she intimated. Rather, it is based upon self-serving claims made by the manufacturers about their own trials of their own products.
Researchers may be “running” subsequent trials, but the regulators do not require evidence from them prior to subsequent “marketing authorisation” of the “tweaked” jabs. The pharmaceutical corporations do not have to “demonstrate” that the jabs work and are safe. They simply have to make claims to that effect, which the paradoxically named “regulators” will apparently accept without any scrutiny whatsoever.
In an effort to “fully explore this complex and deeply divisive debate” about the COVID-19 jabs, neither the BBC nor Prof. Fry felt it was necessary to even mention, let alone discuss, any of this.
Ignoring Fertility and Fetal Health Concerns
Fry enlisted from the British Medical Association a GP who specialises in vaccine promotion to speak to a participant called Ethan about his concerns over male fertility. The doctor told Ethan:
All the research studies that have been done have shown that there is no impact on fertility in male or female patients. However, there have been recent studies and clinical evidence to show that if you have had COVID-19 infection that can, temporarily, effect sperm quality and count.
This was a partly false statement from the GP. A recent study from Israel does show a temporary reduction in male fertility following the Pfizer jab. The scientists concluded:
This longitudinal study focused on SD demonstrates selective temporary sperm concentration and TMC deterioration 3 months after vaccination followed by later recovery.
Another participant in the BBC program, Naomi, was concerned about female fertility. She spoke to the same BMA GP. The GP acknowledged that studies have shown a disturbance in the menstrual cycle following vaccination. The BBC broadcast the doctor telling Naomi:
There are no longstanding issues or effect on fertility.
This statement was seemingly made in reference to the menstruation studies. We don’t know what other advice the GP gave Naomi.
As yet, the jab’s impact upon female fertility is unknown, but there are significant reasons for concern. There was no scientific basis for the BBC to broadcast the claim that there are no “longstanding” fertility issues. On the contrary, the BBC appeared to have once again deliberately misled viewers.
During its pre-clinical trial research, Pfizer found that the lipid nanoparticles (NPs) used in its COVID-19 jabs freely moved around the body. But Pfizer didn’t make this known prior to the shot’s subsequent “approval.” The NPs accumulated in the liver, in the adrenal glands, in the spleen and in both the testes and particularly in the ovaries.
The “long-term” effect of the NPs on fertility may not be established, but there are solid grounds for concern about toxicity, which numerous studies have highlighted. A 2017 review article of these studies noted:
Females are particularly more vulnerable to nanoparticle toxicity, and toxicity in this population may affect reproductivity and fetal development. Moreover, various types of nanoparticles have negative impacts on male germ cells, fetal development, and the female reproductive system.
Dr Luke McLindon, President of the Australasian Institute for Restorative Reproductive Medicine, the primary investigator for numerous clinical trials and the senior obstetrician and gynaecologist for Mater Health in Brisbane, is no longer listed as an employee of Mater Health and has reportedly been sacked.
Why? It seems he was trying to release research data showing that miscarriage rates among his patient group had climbed from a usual maximum of 16% to as high as 74% for his vaccinated patients. This has yet to be confirmed by Dr McLindon, but if his data is correct it only adds to existing concerns.
NP accumulation in the ovaries, as highlighted by Pfizer’s own research, has been worrying scientists for years. The BBC’s disinformation, clearly intended to encourage pregnant women to get the jabs, was potentially dangerous.
Two participants, Chantelle and Naomi, were later taken to visit Prof. Asma Khalil, who told them:
We know for sure that the vaccine does not cause miscarriage. We know that the vaccine does not increase the chance of stillbirth. We really have good safety data from a very large number of women who have received the vaccines. [. . .] There have been no concerns so far. [. . .] Potentially the vaccine is potentially useful for you and the baby. The most recent data tells us that the vaccine could reduce the risk of stillbirth by about 15%.
Prof. Fry backed up Prof. Khalil’s statement:
If you catch COVID while pregnant, your risk of losing the baby to stillbirth is 15% lower if you have had the vaccine.
To which Prof. Khalil added:
We have found that the vaccine, given to pregnant women, prevents hospitalisation because of COVID in the infant for the first 6 months of age.
For reasons we will discuss in Part 2, these statements from professors Fry and Khalil should be viewed with extreme caution. There are disconcerting signs of infant mortality after the jab that require explanation. These concerns were not reported in “Unvaccinated with Professor Hannah Fry.”
In the history of the US Vaccine Adverse Event Reporting System (VAERS), which began monitoring possible vaccine-related AEs in 1990, there have been 2,243 recorded miscarriage and fetal death events potentially linked to the US vaccination schedule over the last three decades. By contrast, in less than two years (2021 and 2022 to date) VAERS has recorded 4,358 miscarriage and fetal events conceivably as a result of the COVID-19 jabs.
Like the MHRA’s Yellow Card system, VAERS is not designed to prove or disprove causality but rather to be analysed to identify concerning “signals.” And, like the Yellow Cards, VAERS captures an unknown percentage of AEs. The US Department of Health and Human Services (HHS) puts it this way:
VAERS receives reports for only a small fraction of actual adverse events.
The HHS, like the MHRA, hasn’t done anything to remedy its known underreporting problem. Its “safety analysis” is just as flawed as the MHRA’s.
Meanwhile, in Scotland, a notable spike in infant mortality occurred in 2021. Despite suggestions that this may have been caused by COVID-19, a subsequent investigation by Public Health Scotland (PHS) found that this was not the case. Another spike was reported by PHS in March 2022:
The neonatal mortality rate was 5.1 per 1,000 live births in September and 4.6 per 1,000 in March, against an average of 1.49 per 1,000 in 2019.
There is a correlation between the vaccine rollout and the Scottish infant mortality spikes. This correlation does not prove jab causation, but any objective investigation should explore the possibility. Dr Sarah Stock, who leads the COVID-19 in Pregnancy in Scotland (COPS) research project, which is partly funded by PHS, said:
I think the numbers are really troubling, and I don’t think we know the reasons why yet. [. . .] What we do know is that it’s not neonatal Covid[.] [. . .] It is very unusual to see these outliers, and understanding why is going to be crucial.
PHS and the COPS project say they do not know what caused the mortality spikes. They are looking at a range of potential reasons to account for these worrying spikes. There is only one potential cause that they have categorically ruled out and refuse to investigate.
When asked if the COVID-19 jabs could have contributed to the neonatal deaths, Dr Stock said that the spikes were:
. . . absolutely not due to the Covid-19 vaccine[.]
Dr Stock and other public health experts claim to have no idea what caused the spikes in Scottish infant deaths. So how do they know that the vaccines are “absolutely” blameless?
We should note that Dr Stock’s work is supported by the Wellcome Trust. The Wellcome Trust has invested £16bn in COVID-19 vaccine development.
The BBC program reported Prof. Khalil’s denial of any reason for concern over neonatal health following vaccination. Perhaps she’s right. Objective scientific research is needed to find out. But if that “science” is produced by the vaccine manufacturers, only an idiot would accept it without serious misgivings about a massive conflict of interest.
The BBC’s so-called documentary was riddled with undisclosed conflicts of interest. Central to its propaganda was an agenda-driven approach to scientific, medical and statistical evidence that would have been apparent to viewers had the BBC been honest about the highly compromised positions of its “experts.”
In its press release announcing the program, the BBC said that Prof. Fry’s academic work “helped bring the UK out of its first lockdown.” In truth, her work contributed towards putting us in lockdown. And not only that, but there is significant evidence to suggest that she was part of a BBC collaboration with the UK government that created the entire, highly dubious concept of a pandemic.
We will explore that and other important issues in Parts 2 and 3.
Propaganda with Professor Hannah Fry







I looked at the data from ukhsa publication for “vaccination” rates (England only) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1088929/Weekly_Flu_and_COVID-19_report_w27.pdf page 65.
The totals don’t add up so I put it into a spreadsheet
Total cohort is 60,296,899 ( adults ie 18 and above) is 50,873,759
Totals Adults Jabbed 1 dose is 41,498,515 (81.57%) no jabs at all 9,375,244 ( 18.47%)
Totals Adults Jabbed 2 doses is 40,033,810 (78.69%) not had 2 jabs is 10,839,949 (21.31%)
Totals Adults jabbed 3 doses is 32,716,541 (64.31%) not had 3 jabs is 18,157,218 (35.69%)
I made a mistake previously by assuming that the totals would add up.
Ps I know that lots of NHS staff have paid to have their details entered onto the database which shows that they are vaccinated when in reality they haven’t had any.
Many thanks David. I’m sure your figures are more accurate so I hope people will check them out. I will asap.
Hi I do not understand what the ramifications are of this statement is: “Ps I know that lots of NHS staff have paid to have their details entered onto the database which shows that they are vaccinated when in reality they haven’t had any.”
I.e. what would be their purpose for doing this.
Do you mean they haven’t had any vaccines or they haven’t had any adverse events from the vaccines?
Can you ellucidate, thanks
Thanks Iain,
I read Pseudopandemic not long after it was published. It is by far the most thorough and comprehensive analysis of the insane situation we have been put in, over these last two and a half years.
As you make clear, it all comes back to the interests of the international corporate raiders and the criminal banking cartel.
Public health? Who cares about THAT!
I greatly appreciate your sterling work in this and other, equally important, fields.
I also think your beard is pretty cool too!
Lol. Thank Nick (I think)
Articles about TV spread official line.
1
Missing info, different situation, different point viewed from, imprecise definition, linguistics, both parties partly incorrect e.g.
Right meaning correct could be left.
Right-hand side of cupboards is on our left-hand side because cupboards face us.
English (UK) uses infection, infectious, contagion, contagious. US uses contagious generally. Long known coronavirus air-born; no controversy, just linguistics.
Nothing known about coronavirus, said IT, psychology, ‘social’, epidemiology; none of which are science.
2
Accepting unproven accusation ‘guilty’ suggests insufficient self-respect, possibly due to insufficient ethical/moral personal values.
Foundation of whole of English Law – first assumption innocent.
WWII’s outcome – birth-right to be free of fear.
‘Panic buyers’ and ‘little Hitlers’ top to bottom inclusive clearly not true-Brits.
3
AE reporting systems are ‘open-label’; not appropriate substitutes for clinical trials.
Double-blind, randomised, rigorously conducted trials cost stratospheric amounts of money. Marketing been wanting clinical research abolished for decades.
Obvious in Dec 2020 clinical research abolished; everything subsequent, untrialled.
4
Some chose to not be jabbed, others to be jabbed; any damage to our physical health resulting from our own choice is our own responsibility.
Adults carry responsibility for the result of their actions.
5
Repeatedly from Jan 2020 to mid-March 2020:
Majority who catch coronavirus (a cold) suffer only mild or moderate symptoms and 99.9% population not at risk from coronavirus.
The virus did not justify jabs for any more than 0.1% of population, if that.
Discussing jabs buries that vital fact.
First – virus going around no danger to 99.9% of population. But
‘Project fear’ – long known to be seriously detrimental to physical health. Then
Restrictions – each of which was known to seriously damage physical health.
And, jabs.
Disentangling which action caused what, what combinations caused what, from repeatedly corrupted database – not possible.
6
Long known, well-established, harm to physical health by fear and every restriction including plastic screens.
Disseminating that info is vital to empower each to assess health-risks from WEFetal’s claims versus health-risks from WEFetal’s actions.
Thereby inhibiting WEFetal’s murderous intent.
AE reports show WEFetal they’re succeeding in their intent.
7
All drugs are poisons.
Not possible for any Pharma product to be 100% safe.
None known does Not mean none.
Unsafe products damage health – our good health is bad for Pharma profits.
So, since 2002 Pharma routinely avoid looking where theory suggests safety issues likely because most hear what they want, not what’s said: ‘no evidence’.
No evidence does Not mean no problem; Nor does it mean effective.
Found nothing does Not mean nothing to find.
Genetically engineered stuff released before equipment sufficiently refined to look where theory suggests dangers may be – no evidence – clean hands bwana, perhaps only until equipment becomes available after geneticists’ own grand-children born.
But:
Although we don’t need TV or jabs, we do need real food.
Thanks Jane
Thanks for the brilliant analysis Ian. I just thought I’d mention that the government has a Patient Information leaflet for the Phizer Vaccine which is here https://www.gov.uk/government/publications/regulatory-approval-of-pfizer-biontech-vaccine-for-covid-19/patient-information-leaflet-for-covid-19-vaccine-pfizerbiontech. In that leaflet it states that the chance of getting Myocarditis is roughly 1 in 10,000. Not sure how they have come to that number. It’s a bit miss leading considering the chance of Myocarditis increases down the age groups. I would be interested to know where Fry for her 1 in 33,000 number is from.
I was stupid enough to go along for the vaccine but came to my senses before they could inject me. I never saw any Patient Safety Leaflet, mention of side effects or the fact that the vaccine is experimental.
I’ll be interested to see your follow-up article. I find it ridiculous that mathematicians were so instrumental in taking us in and out of lockdown with their laughable models. I wonder hows Fry’s models compare to Ferguson’s.
Thanks Jonathan. All will be revealed. You won’t believe it.
I had enough of a reaction to the vaccine to seek medical advice and be referred to a specialist. With the delays in being referred, and then to get an appointment, it was 6 months before I saw him. Even though I was still suffering symptoms after that much time I was told I was only suffering a “normal reaction” to the vaccine. I was told to meet the criteria for having had an “adverse event” officially recorded I had to be unable to walk. So for a “case” of covid I only had to test positive. It was still an officially recorded case of covid even if it was completely asymptomatic. But for a case of an adverse event from the vaccine to be officially recorded I had to be hospitalised. If that isn’t rigging the statistics on how safe the vaccines are, or aren’t, by denying any adverse events were anything more than a normal reaction unless they were life-threateningly serious, I don’t know what else you’d call it. It took me nine months to fully recover from what was officially described as a normal reaction to a very safe vaccine, one we know is because look how few adverse events have been officially recorded.
Thanks Gordon and sorry to hear about what you have been through. I couldn’t agree more on how the statistics have been managed and reported. It seems to me that if death within 28 days of a positive test is recorded and reported as a COVID-19 death, then a death within 28 days of a jab should be recorded and reported as jab related. The way the stats have been manipulated is, in itself, evidence of a wider agenda.
I’m not a covid denier. Covid is real. The vaccines benefit most people. I don’t think there’s an evil conspiracy to rig the numbers. Just a lot of sincere good people who want the numbers to say what they think the public needs to hear, that the virus is very bad, and the vaccines safe. I went and had the vaccine. And only became a critic when I personally experienced what happens when you try to tell medicos that you suspect you are one of the people the vaccine wasn’t safe for. First I went to my GP. He looked for something he was familiar with, and when it wasn’t, he just gave up. Then when it got worse and I had the audacity to go to the internet – the medically reputable part of it – and come back with a possible diagnosis that it was a vaccine-related adverse event he just ridiculed it. It took going to another GP to get a referral to a specialist. And of course with all the relevant specialists very busy because of the pandemic that took months. The official diagnostic criteria was that for it to be signed off as a vaccine related adverse event was that it had to be signed off by a specialist that it was proven it wasn’t caused by anything else. In actuality because so much time had passed I had largely recovered, so he did no examination, no tests and asked no questions. I can’t count the number of times I’ve had postings deleted as anti-covid fake facts because I pointed out that the count of covid deaths isn’t of people who died (primarily) of covid, but anyone who tested positive within 14 days of death, or at death, or even just died with symptoms consistent with covid. Good people with good intentions can all too easily become zealots who see it as doing the right thing to make the numbers say what they think they should.
You only have to look at “long covid”. There is no doubt its real to some degree. It is normal for people who have suffered any serious medical condition to suffer some related after effects for a while. But its also normal for people to connect every little bad symptom, real or imagined, that they suffer for a long time to that condition, whether they are connected or not. And I don’t want to sound like I’m sexist, but the fact that far more women say they they are suffering from long covid than men, which rings alarm bells because there’s no obvious biological reason. And it is an established scientific fact that women are more susceptible to “mass hysteria” than men. That when they are told other people have suffered something, they become convinced they have too. Me too. You can put it down to being more empathetic if you like.
Thanks so much for your comment Gordon. I don’t think anyone who questions what I call the pseudopandemic is a “covid denier.” There are those who argue that virology itself is a quack science and that viruses do not exist. I do not agree with that view and, like you, I consider COVID-19 to be a real disease that has impacted people. However, “denial” suggests a refusal without reason and has obvious connotations to “holocaust denial”. It is used as a pejorative to label people as “other” fo their views. Even those who claim viruses do not exist have good reason to make that claim and offer evidence to back up their argument. That does not make their claim a “fact” but we need to look at all evidence and assess and debate it to find the facts. When labels, such as “covid-denier,” are used to shut down debate then that is suggestive of an agenda pursued by those who refuse to debate the evidence.
I also believe that the overwhelming majority of the people who push the COVID-19 narrative absolutely believe what they are saying is true and defend that narrative with the best of intentions because they think it is important. They have a real and genuine concern for public health. However, when that extends to massaging data again I suspect and agenda.
Those of us who question the COVID narrative, in my experience, also do so out of a genuine concern for people’s welfare. If you do not believe that COVID-19 presented an existential threat then the response measures (lockdowns, biosecurity, social distancing, etc.) cuase a threat to public health. We already know what impact these have had on vital health screening, waiting lists, mental health, inequality of opportunity, the economy, acces to primary care for the most vulnerable and more damages besides. Excess martality remains consistently high and most of it is not due to COVID. These concerns are also legitimate and do not suggest any “denial.”
It is when we step back and look at the wider political and even geopolitical context that a clear possible “agenda” emerges. This too needs to be investigated, the evidence examined and people informed about why the pseudopandemic meets the goals of those who would claim to rule us. Again this does not mean that all can be stated as fact, but unless we look at the evidence, if such an agenda exists, we allow the possible perpetrators to get away with it unchallenged and suffer the consequences as a result.
I totally agree that every single claim should be backed up by a strong amount of evidence to make it a fact. The claim that the Earth is flat is also explained by a good amount of reasoning even evidence was presented that it’s “definitely not rounded” but can we actually state is as a fact that the earth is flat 🤔
Thanks Sergei. All the evidence has to support the theory for it to be sound. Despite Sagnac and Michelson-Morley, I would say that there is a lot of evidence that the Earth is a globe wouldn’t you?
…Well, oblique spheroid at least.
I think it’s a globe yes and I’ve never been a flat earther. Not sure if the “evidence” of the flat earth is strong enough. Some of my mates are too carried away by alternative narratives so they think that literally everything we’ve been taught is a lie.
The flat earth perspective is an interesting one, not that there is any convincing evidence that it should be a widely held belief, however if you were transported back in time, pre-enlightenment and were tasked with the challenge of explaining that the earth is spherical not flat, then the majority of people would struggle to do this. Even at the top of a mountain, it is difficult to see the curvature of the earth.
This is not an argument in support of the ‘flat earth’perspective, but people so often rely upon the information that they are told is true and correct, that they lose track of what is plainly there to see right in front of them!
I don’t personally know anyone that was severely affected by covid, equally I do not know of anyone who has suffered adversely from the jab, but it has not stopped me forming an opinion on whether the ‘pandemic’ was real or contrived, despite a lack of first hand evidence!
When it is not possible to make a conclusion based on the evidence in front of us, it is critical to gather as much information from many sources to create an informed view.
As such, the ‘flat earth’ tag is possibly best aimed at those who refuse to believe anything other than that which they can see first hand, rather than a belief in outdated and disproved theories.
One point overlooked with regards to “nocebo” effect is that it is always assumed that the placebo given is inert.
In many documented cases this is patently untrue, the exact contents of a placebo pill are often unknown; the “recipe” is not disclosed to the trial subjects, nor is it published in the peer-reviewed literature.
As an example:
In trials of the human papilloma virus (HPV) vaccine, participants were told they were either receiving a “vaccine or placebo.” The vaccine manufacturer defines a placebo as an “inactive pill, liquid, or powder that has no treatment value.”
However, participants in the placebo group did not receive an inactive substance of no treatment value. “Instead,” RIAT researchers state in the BMJ, “they received an injection containing amorphous aluminium hydroxyphosphate (AAHS), a proprietary adjuvant system used in the Gardasil vaccine to boost immune response.” – Source https://www.crossfit.com/health/sometimes-a-placebo-is-not-a-placebo
Thanks John, Yes the so-called HPV trials were a disgrace. I wrote about them here if you are interested: – https://iaindavis.com/vaccines-part-4/
In the reference meta-analysis they specifically stated that studies were selected for analysis because they used “inert saline” placebos. I didn’t dig into it further, but like you I doubt that is the case in every instance.
I have only just read this excellent article by Iain, but by coincidence, have also today received an email about data from Israel indicating that menstrual problems after the “vaccine” may not always be short term.
“The findings show, among other things, that adverse events are 2-4 times more common among young children aged 5-11; that there are new adverse events that have not been reported in Pfizer’s COVID vaccine leaflet; that contrary to what has been claimed, various adverse events, including neurological effects and menstrual disorders, are not short-term events that pass within a few days, but in many cases, they last for months or even more than a year. Moreover, the study found that a significant proportion of the symptoms did not disappear by the end of the study, so it is not possible to know how long they lasted; and a considerable part of the cases even if the adverse event ceased, it recurred after the next dose”.
https://lionessofjudah.substack.com/p/breaking-the-israeli-moh-is-hiding
Thanks Alison. Interesting developments. Thanks for bringing it to my attention.