
[Disclaimer: I am not medically qualified. If you feel ill you should always seek medical advice and should not take medication without medical advice.]
In Part 1 we looked at the reasons why chloroquine, particularly hydroxychloroquine, has become a strong candidate for the possible preventative treatment of the COVID 19 syndrome caused by the SARS-CoV-2 (SC2) coronavirus. We assessed some of the claims and counterclaims made, and questioned if the focus upon developing a vaccine, at the apparent expense of exploring more immediate treatment options, makes sense in the circumstances.
Now we’ll consider what appears to be a deliberate campaign to avoid trialling hydroxychloroquine. Who has potentially been involved and what factors may explain this strange opposition? Before continuing, if you haven’t yet done so, please read Part 1. This post assumes you are aware of the issues raised in that article.
The Chloroquine Fact Checkers
Following Prof. Dider Raoult’s vocal support of the Chinese researchers and chloroquine’s potential, Le Monde’s fact checking Décodeurs began to release headlines like “Coronavirus Hydroxychloroquine: The Buzyn-Levy Couple, Target of Misleading Publications.” The article rightly questioned the tendency of some to make conclusive statements based upon assumption and suspicion. However, in their “nothing to see here” piece, les Décodeurs went to great lengths to insist these suspicions were all a “conspiracy.” They stated:
“The technique is well known: mixing real information with diverted or even invented facts.”
Just as Le Monde’s Décodeurs did when they worked with Facebook to block access to a video published by the Mediterranean Infection Institute (IHU). As one of Facebook’s official fact checking partners, les Décodeurs explained why they considered Prof Raoult’s opinion to be “fake news,” worthy of their censorship:
“Professor Raoult’s announcement is based on a very short “letter” to the journal BioScience Trends February 18 and published online the same day. Three researchers from the city of Qingdao (east China) mention ongoing clinical trials in more than ten Chinese hospitals.”

Stating Prof. Raoult’s announcement is based on a short letter is an “invented fact.” As is the false claim that Chinese researchers “mention” ongoing trials. The letter was written in English because the Chinese scientists obviously wanted to release their data as widely and as quickly as possible. Perhaps les Décodeurs overlooked the apparent global pandemic?
In the letter the Chinese scientists provided references to completed clinical trials. Prof Raoult’s opinion is based on the data. Like any other scientist in the world, he could access the evidence. I’m sure his years of experience, as one of the worlds leading microbiologists, also helped him form his opinion.
To be fair to les Décodeurs, they weren’t the only fact checkers who decided advice from world renowned scientists was “fake news.” AP Fact Check, in response to Donald Trump’s observation that chloroquine could potentially bring infection rates down, said:
“The drugs he is referring to [hydroxychloroquine] are for treatment in patients already infected. That doesn’t prevent spread of the virus.”
This is not a fact, it’s “wrong.” If chloroquine performs as initial trials suggest, it will reduce viral load and duration of infection in patients already infected. This means they won’t be shedding the infection as readily, which will reduce the spread of infection.
Approved fact checkers have other ways of spinning the truth. Disinformation by omission being one. On March 19th Factcheck.org, speaking about progress in China stated:
“It is currently being tested in clinical trials in China, where it is included in government guidelines for treating coronavirus patients…….if the drug show promise, the FDA says it will engage with domestic manufacturers to ramp up production of this product.”

In common with many others, this fact checker forgot to mention that limited trials were completed, which is why chloroquine entered into treatment guidelines. Nor did they mention its apparent efficacy in clinical settings. By questioning “if” the drug will show promise they deceived the reader into believing it hasn’t already shown promise, which it has.
In 2017 the global advertising giant WPP’s European group M/Mindshare were contracted as the media agency for Sanofi. Managing Sanofi’s vast advertising budget outside of the U.S. This move followed their significant 2014 investment in Les Nouvelles Editions Indépendantes (LNEI), the European media conglomerate created by Matthieu Pigasse. Along with business partners Daniel Kretinsky and Xavier Niel, Matthieu Pigasse owns “Le Monde” and pays the wages of Les Décodeurs.
Is it reasonable to ask why these corporate owned MSM fact checkers have been so loose with their claimed chloroquine facts? Why have they not been encouraged by the prevailing science? Why have they apparently sought to mislead the public?
Chloroquine Fake News
Alleged fact checkers are not the only prominent voices to have spread a little “fake news” about chloroquine, and in particular hydroxychloroquine. Speaking on March 24th the new French health minister Olivier Véran told the public:
“Cardiologists are also warning me that hydroxychloroquine can cause heart problems. In the United States, today, a person who had used it in self-medication suffered a fatal cardiac arrest.”
While it is wise to caution against non prescribed use of medication, again some disinformation crept in. There’s a pattern forming here. Someone doesn’t like chloroquine.

The heart risk from chloroquine is not clear. Indeed some meta analysis of related studies indicate it may be associated with reduced cardiovascular risk in some patients. Where those risks have been suggested they are associated with acute poisoning, often deliberate, when used in combination with other antiviral drugs like lopinavir, or with prolonged use, not when used appropriately in short courses of treatment for specific syndromes such as COVID 19.
Amid the consistent fear porn and disinformation poured out by the mainstream media, an Arizona couple drank fish tank cleaner because it contained chloroquine. Needless to say this was not “self medication” with hydroxychloroquine tablets. This sad incident says far more about the immense fear the population is labouring under than it does about legitimate scientific and clinical research.
For the most senior officials to suggest people have died in the U.S after using hydroxychloroquine, as prescribed, is disinformation. Perhaps the French Health Minister was simply mistaken? He could have been more careful.
Eight weeks after chloroquine evidence first emerged, Olivier Véran allowed treating physicians to use it “off label” for COVID 19 treatment. Doctors are free to use it as they deem appropriate, but only for the most seriously ill patients. This guidance, though welcome, is still incongruent with the existing clinical recommendations to treat less severe cases.
If the French state is now willing to allow its use, while further clinical results are pending, why weren’t they willing to base that decision on the existing science? In terms of possibly slowing the pandemic, or “flattening the curve”, Véran’s decision made no sense.
Wider use would possibly reduce viral load and illness duration, inhibiting the spread of infection. Potentially making the need for a vaccine less urgent and the necessity for a global economic shutdown redundant. Yet there seems to be very little enthusiasm among some establishment figures, in France and elsewhere, to pursue this option. Could this explain the opposition to trialling chloroquine? Do some powerful forces want the lock down to persist? Is a vaccine the only end point allowed?
Despite Le Monde’s insistence the State is beyond suspicion of corruption and obstruction, legitimate questions should be asked. While their fact checkers note powerful voices in the French state may have acted to discredit chloroquine researchers, they stress these are merely allegations, “yet to be proven.”
Quite so, and it is supposed to be the role of the mainstream media, like Le Monde, to investigate such allegations. But they haven’t. Rather than questioning power they have staunchly defended it. We wait to see if they will actually interrogate any of the evidence. In the meantime, it is left to the alternative media to do so. They do it knowing the MSM will immediately castigate them as conspiracy theorists.
Questioning power at all is practically the definition of conspiracy theory. It used to be the definition of journalism.
Chloroquine Objections Run Deep
 The inexplicable resistance to trialling chloroquine has been persistent. On 25th March Le Monde’s Décodeurs Published an article in which they alleged that Prof. Didier Raoult had offered a “miracle cure.” They decried his opinion as “at best fragile, at worst wobbly” adding, “we are starting to count the first victims – by intoxication – of the craze for this molecule.” Insinuating Prof. Raoult should shoulder blame for causing the craze and alleged associated deaths. Though what he can do to stop people drinking caustic cleaning fluid isn’t entirely clear.
The inexplicable resistance to trialling chloroquine has been persistent. On 25th March Le Monde’s Décodeurs Published an article in which they alleged that Prof. Didier Raoult had offered a “miracle cure.” They decried his opinion as “at best fragile, at worst wobbly” adding, “we are starting to count the first victims – by intoxication – of the craze for this molecule.” Insinuating Prof. Raoult should shoulder blame for causing the craze and alleged associated deaths. Though what he can do to stop people drinking caustic cleaning fluid isn’t entirely clear.
Les Décodeurs then released a video in which fellow scientist Professor Karine Lacombe appeared to suggest Prof. Raoult was recommending people take the drug contrary to medical advice. Whereas, in reality, he was advocating rapid repurposing trials. The video harshly criticised Prof Raoult’s trials for lack of rigour. This was reasonable, Raoult’s team admitted this themselves, saying they had, contrary to common practice, released preliminary results precisely because this is not a normal situation.

Explaining the lengthy clinical trial process, the Décodeurs acknowledged trials can run faster in emergencies, especially when the trialled drugs safety profile is already well known. Hydroxychloroquine’s well known safety profile wasn’t mentioned. Instead, Le Monde merely noted it had been available for many years. Misleading viewers into imagining the unknown safety of hydroxychloroquine.
In a moment of bewildering disinformation, Le Monde then stated “no human trials have been successful.” Nowhere, in their well promoted video, did Le Monde acknowledge that Prof Raoult’s first trial was essentially a corroborative investigation of the Chinese clinical trials. Nor do they mention his team clinical results, nor that China, South Korea and others have apparently been successfully treating COVID 19 patients with chloroquine.
Calling the conduct of the Prof. Raoult’s team “absolutely scandalous” Prof. Lacombe, chief of the Department of Infectious Diseases at the St-Antoine Hospital (AP-HP), accused them of being “outside any ethical approach.” As yet she hasn’t levelled the same accusations against the WHO’s SOLIDARITY trials, though they won’t be using the double blind standard either.
Prof. Lacombe is a grant recipient from Gilead Sciences who hold the patent for their experimental drug remdesivir, currently being trialled as a potential COVID 19 treatment by the French Institute of Health and Medical Research called Inserm. She is one of Inserm’s leading authors and a frequent lecturer on the French University Hospital (CHU) circuit.
AP-HP, where Prof. Lacombe heads a research department, currently holds more than 650 medical patents and has just announced a public private research partnership, in collaboration with the French government and the global pharmaceutical giant Sanofi. Her department will receive money from the seed fund set up by Sanofi. Speaking of their pride in the potentially lucrative collaboration, Sanofi announced:
“In light of the scale and urgency of the COVID-19 epidemic, Europe’s biggest university hospital center AP-HP and France’s leading pharma firm Sanofi, are joining forces to speed up clinical research to stem the epidemic……Since the outbreak of the epidemic, Sanofi has tirelessly continued to apply its knowledge of vaccines in particular…..sharing its experience with other countries in the research and development of vaccines with the CEPI (Coalition for Epidemic Preparedness Innovations).”
Sanofi, along with Gilead Sciences, are one of the many industry partners of Inserm. Inserm’s investment arm is called Inserm Transfert . It is a public private partnership and holds 82 license agreements and 300 R&D agreements with pharmaceutical corporations.
Sanofi also partners with CEPI and has a “non voting” seat on its Scientific Advisory Committee (SAC.) CEPI are focused exclusively on producing a coronavirus vaccine seeking $2 billion tax payer investment to create one. They are partnering with Inserm in the vaccine hunt. CEPI was created by, among others, the World Economic Forum, the Bill and Melida Gates tax exempt foundation and GlaxoSmithKline’s tax exempt foundation the Wellcome Trust. Bill Gates personal net worth alone is estimated to be $102 billion.
Chloroquine The French Connection
Following a recommendation made in November 2019, on January 15th then French Minister of Solidarity In Health, Agnès Buzyn, reclassified hydroxychloroquine in all its forms as a poisonous substance. It is by no means clear why a medication, available over the counter in French pharmacies for more than 50 years, with a proven safety profile, should suddenly be made solely available on prescription.
 It is probably just a coincidence that the French state happened to limit access to the only freely available drug that would shortly become the first in the world to potentially offer a preventative treatment for a global pandemic. A pandemic for which the World Economic Forum, who formed CEPI, have an incredibly extensive and well prepared Strategic Intelligence plan.
It is probably just a coincidence that the French state happened to limit access to the only freely available drug that would shortly become the first in the world to potentially offer a preventative treatment for a global pandemic. A pandemic for which the World Economic Forum, who formed CEPI, have an incredibly extensive and well prepared Strategic Intelligence plan.
Similarly, it is probably just another remarkable coincidence that CEPI is working with Inserm, the French State and its own board member Sanofi, to develop the vaccine the world is clamouring for. Hopefully $2 billion in European tax revenue will help in this corporate and private foundation led effort.
Agnès Buzyn ministerial role included oversight of Inserm. Eyebrows were raised when her husband Yves Lévy was appointed its head in 2014, during her period in office. Despite the glaringly obvious conflict of interest, and a nominal decree in 2017 that Agnès Buzyn would have no further control of Inserm, the husband and wife team were nonetheless responsible for both French health policy and medical research for the 4 years.
Yves Levy left Inserm in 2018 to become a special legal adviser to the French Council of State, though he has no notable legal experience. Agnès Buzyn resigned her ministerial post, in the midst of the emerging coronavirus pandemic, on February 16th 2020, supposedly to pursue her ambitions to run for Paris Mayor.
Prior to his new role, Yves Lévy greatly improved Inserm’s vaccine development capabilities. As the former scientific director of the French National vaccine programme and executive director the Vaccine Research Institute laboratory of excellence, he was well suited to the job.
On the March 11th, five weeks after the first indication that chloroquine would be worth trialling for SC2, decades after it’s potential to treat SARS-CoV was clear and three weeks after initial clinical trials results reinforced the likelihood, the French government’s health emergency rapid response committee (REACTing – REsearch and ACTion targeting emerging infectious diseases) announced they would exclude chloroquine and would only trial the patented drugs.
Professor Yazdan Yazdanpanah, head of REACTing, stated:
“We have not retained it [chloroquine] for the moment, in particular because of its undesirable effects. It also has frequent interactions with other drugs. However, intensive care patients are often treated with multiple drugs.”
REACTing is a committee of Inserm.
 Following considerable public outcry, primarily as a result of Prof. Raoult’s high profile championing of hydroxychloroquine, in a dramatic u-turn, on March 24th Inserm announced extensive clinical trials of potential COVID 19 treatments to include hydroxychloroquine.
Following considerable public outcry, primarily as a result of Prof. Raoult’s high profile championing of hydroxychloroquine, in a dramatic u-turn, on March 24th Inserm announced extensive clinical trials of potential COVID 19 treatments to include hydroxychloroquine.
Initial completed trials of lopinavir & ritonavar have shown no beneficial therapeutic effect. Hopes may now hinge on Gilead’s remdesivir and the ‘off patent’ hydroxychloroquine. It is the only drug in the trials for which both completed clinical trial and successful COVID 19 treatment data already exists.
The trials are expected to take at least six weeks. Results could be available about three and a half months after Chinese researchers first alerted the world that chloroquine could possibly treat COVID 19. We wait to see if Inserm will approve their industry partner’s remdesivir or the off patent hydroxychlorine. Hopefully they’ll approve all the drugs that work. It is possible none will.
Although distinctly hostile to the chloroquine data for months, Inserm stated, in their press release dated the March 22nd:
“We analyzed the data from the scientific literature concerning the SARS and MERS coronaviruses as well as the first publications on SARS-COV2 from China to arrive at a list of antiviral molecules to be tested: remdesivir, lopinavir in combination with ritonavir…..and hydroxychloroquine. The list of these potential drugs is also based on the list of experimental treatments classified as priorities by the World Health Organization.”
Better late than never. Shame about the totally unnecessary delay.
Given the comments of officials and high ranking physicians, apparent commercial conflicts of interest, fake facts from fact checkers and inexplicable clinical and regulatory decisions, a consistent disinformation campaign against chloroquine is evident. Further, the commercial conflicts raise the sickening possibility that profits, not lives, have in part driven this agenda.
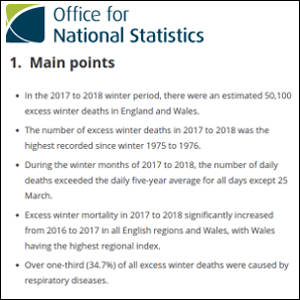
While there is currently no evidence that excess winter mortality is anywhere near as bad as it was in 2017, the economy has been shut down and we all remain under effective house arrest. It would be extremely foolish to ignore evidence that suggests a degree of manipulation. All we can hope is that effective treatments will be found and that the economic damage isn’t too severe. Unfortunately that is not looking very likely.







Excellent series of articles! You’re incredibly thorough.
Regarding the Discovery clinical trials, it transpired that the hydroxychloroquine + azithromycin combo will only be administered to “terminal” patients with severe respiratory issues. Since that treatment is most efficient within the first 8 days of infection, we can safely guess that the Discovery report will conclude that chloroquine is inefficient in treating covid 19 patients and maybe even precipitated their deaths. (I couldn’t find a source that isn’t behind a paywall, but the info is out there)
Also, the WHO itself signalled that Remdesivir was the only efficient drug, which made Gilead’s stock go through the roof. Maybe it’s just me, but I find the timing interesting, since the WHO’s declaration came out maybe 24hrs before Raoult went public with his protocol on youtube on Feb 25th.
https://edition.cnn.com/2020/02/24/investing/gilead-sciences-coronavirus-who-remdesivir/index.html
Similar to that apparent unanimity on Remdesivir, I also find it a bit odd to see every Western health authorities turn almost simultaneously to Palantir to manage their population’s covid data. But again, maybe it’s just me.
Keep up the good work! And stay safe. Figures may be overblown and the crisis engineered/exploited to a certain degree, but the virus is very real and it can hit really hard.
Thanks for the fascinating comment and the encouragement is much appreciated. I agree the virus is real and it is clearly a nasty coronovirus strain. My question, is it an unusual or rare strain of coronavirus? I am less convinced on that. I am following the self isolation and social distancing protocols which seems a sensible precautionary measure to me. Like you I have very little faith that chloroquine will ever be “fairly trialled.” We wait to see, but clearly the French in particular, and through Inserm the WHO, do not want chloroquine to be a successful treatment. I wonder if this has something to do with the fact that it has long been known as a potential effective treatment for the SARS strains. Suggesting both that there was no desire to find a treatment and that SARS-CoV-2 is not as novel as they would like us to believe.
And it should come as no surprise that chloroquine and derivatives might be effective in the treatment of a corona virus, see this paper from 2005:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1232869/
This was just after the SARS-CoV panic (a very similar corona virus), and this study looked at the performance and potential mechanism of action for chloroquine. Not only that, but also a potential rapid test due to the “indirect immunofluorescence” observed – I wonder how the accuracy compares to those far from flawless RT-PCR tests…
The study was only in vitro (i.e. in a dish in the lab) but it’s no surprise why at least some doctors looked to this family of compounds as a potential treatment.
It really is a shame that chloroquines are so cheap, so well understood and so widely available otherwise we’d all be back at work by now… I guess we’ll just have to wait a year or two for that rushed, barely tested but pricey vaccine…
A hat tip to Del Bigtree on youtube for bringing this one to my attention: https://www.youtube.com/watch?v=7hvkq-R1QGU
Keep up the good work!
Thanks Despair Squid. I think you may have revealed why chloroquine wasn’t the first “go to” and obvious drug to trial with your observation:
One thing you have not mentioned (and which is almost never mentioned). The efficacy of HCQ is based on it being a zinc ionophore, that is, it gets zinc ions across the cell membrane, where it purportedly suppresses the enzyme activity of RdRp (RNA-dependent RNA polymerase). An interesting 2010 science article on the mechanism can be found here: https://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1001176
HCQ should be combined with zinc sulphate supplements. The Chinese studies looked at variable results for a cocktail of HCQ, zinc, azithromyacin, and remdesavir, concluding that combining them led to better results than any of the components separately.
The way things are going it wouldn’t even surprise me if clinical trials left this part of the equation out, in an attempt to prove it doesn’t work.
Another thing that has astonished me is that the CDC has to have statistics on millions of lupus/rheuma patients people already using HCQ. Anecdotally physicians tell of prescribing this for them (as well as travellers to malaria regions) without caveats or significant monitoring, and the CDC should have statistics on the safety profile. C19 disease progression of these patients or evidence of prophylaxis may be garnered from statistics without starting new clinical trials. Don’t expect the CDC to be forthcoming.
I’m am having difficulty understanding the zinc+hydroxychloroquine thing. This drug has been around for 80 years, is prescribed routinely for malaria, is used by lupus and rheuma patients for years on end with no significant monitoring or caveats, and everybody is just so concerned that we do not know if it is harmful. More harmful than landing up in the ICU with Corona and intubation? Where is the concern about the harm of sedation + intubation (orders of magnitude worse than zinc+chloroquine to not get there). The Chinese and South Koreans included it in their standard therapy guidelines months ago. It is being used all over (scores of hospitals and doctors). Billions being spent on the thin and unlikely hope for a vaccine, which everyone is touting as the final solution.
It seems as incomprehensible as the Russian interference ghost.
When my wife came down with C19 (infected at the old-age home where she works; for both of us it’s now in the rear view mirror), I sent her to the doctor with a recipe and emphasized that this is more effective early in the disease progression:
Azithromycin 500mg 5days @1/day
Hydroxychloroquine 200mg 5days @2/day
Zinc Sulphate 220mg 5days @1/day
The doctor said no-can-do. No alternative or therapy offered. No test, because she had a fever (2 weeks later she did get a test after 3 false starts, b/c they were testing the staff). They were set on doing nothing rather than prescribe $20 of common medicines, potentially risking her life. This is how the medical industry is set up. In the nineties they introduced “evidence-based” therapy [pretty late in the game, I would say], and I am told by a brother and sister (both surgeons) that all kinds of standard therapies are not based on evidence, but if you don’t do them, you can be in big trouble. Have you ever seen a GP consult a book if he doesn’t know something for sure? A friend of mine (psychiatrist) used to say: Medicine is a study for dumb people. He didn’t mean that it is easy. He meant you will get ahead if you just do as you’re told unquestioningly. Medicine is more based on authority than Medieval scholasticism (before experimental science) ever was.
Incidentally, when I asked end of February (when I was wiping down the door handles and elevator buttons with disinfectant at my office, to very strange glances) what measures they had at this old-age home, there were none! All measures came at least 3 weeks too late, and in too lackadaisical a manner to be effective. We already knew from the Chinese and the Italians that >98% of the pool of patients landing up in the ICU were aged with comorbidities. We should have sealed these people in and quarantined other vulnerable parties until the virus burns its way through the population, pay the nursing staff a bonus of $K50 to camp inside (quite a bit cheaper than spending Trillions). You put criminals in a jail house; you don’t confine the entire population in a safe house.
Excellent & real fact checkers!
Congratulations for the amazing work!
May I add several info?
There is a personal conflict between former French Minister of Solidarity In Health Agnès Buzyn’s husband Yves Lévy (Inserm), it also explains a lot (it is mentionned by “les décodeurs” of Le Monde, but Les Décodeurs is a false fact checker if not a propaganda tool).
Concerning the “lack of rigour” of Dr. Raoult, he did not really admitted it (and if you look at his scientific curriculum you’ll doubt such a researcher may not be rigorous), but he clearly stated he made the choice “to heal people, not to do researches” (while he and his team are also progressively publishing their results at the same time). He also noticed that most critics were coming from doctors who were no practising (healing) any more for years…
And thank you for noting this disturbing fact: “Following a recommendation made in November 2019, on January 15th then French Minister of Solidarity In Health, Agnès Buzyn, reclassified hydroxychloroquine in all its forms as a poisonous substance…”
Thanks Amadis very useful information.
My understanding is the same as J W Rebel. Hydroxychloroquine should definitely be given with zinc. Just need a very low dose HCQ, to get the zinc into the cells.
Most studies seem to be designed to pretend HCQ does not work: they do not give zinc, & sometimes give stupidly high doses HCQ. Some studies even used vitamin C as the control – so they obviously know that vitamin C is a brilliant anti-viral!
Zinc deficiency is prominent in diseases of aging and in illnesses associated with immune compromise. Of course all nutrients are critical, but there is a striking similarity between zinc deficiency symptoms to those of COVID-19 , including loss of sense of taste & smell.
Dr Thomas Levy says Chloroquine/ Hydroxychloroquine “is the most impressive therapy I have ever seen in treating near-death ARDS patients with coronavirus, and requiring mechanical ventilation. Unless a patient is ready to expire imminently, chloroquine can be expected to bring about recovery practically 100% of the time. It’s equally impressive as hydrogen peroxide for resolving early pathogen colonizations, coughs, and colds (and probably for all respiratory viruses, not just coronavirus). It’s been around for 80 years, and at the low advised doses, is virtually side effect free. Chloroquine is an IONOPHORE. An ionophore is a chemical species that reversibly binds ions. Many ionophores are lipid-soluble entities that transport ions across a cell membrane. Chloroquine is a well-documented zinc ionophore. By itself, zinc does not readily cross the cell wall and enter the cell, largely because it is ionically charged. INTRACELLULAR zinc is a potent inhibitor of viral replication, appearing to interrupt the RNA polymerase that the virus needs to continue its multiplication. While many people promptly recover from all stages of coronavirus infection with just chloroquine, it is a good idea to include 40 to 50 mg daily of zinc supplementation (no more than 30 daily indefinitely when there is no pandemic). My personal opinion is that if the US promptly supplied every adult with five 500mg capsules of chloroquine, to be taken one daily, the entire pandemic in the US would be over in seven to 10 days.” (Dr Thomas Levy https://www.peakenergy.com/index.html )
https://www.youtube.com/watch?v=i4fo13Ss3VQ&feature=youtu.be
Dr Levy c19 INTERVIEW
https://articles.mercola.com/sites/articles/archive/2020/04/20/zinc-dosage-for-immune-system.aspx How to Improve Zinc Uptake with Quercetin to Boost Immune Health
So frustrating if UK has lots stocks HCQ but they won’t let us use it. Are they saving it to give us when the vaccine comes out, so they can pretend the vaccine worked?
Thanks Sumy for an informative and well researched comment. This is particularly relevant to a post I am currently working on, so many thanks for your valuable assistance. If, as you say, the State has withheld an effective treatment, then it tells us much about the approach to public health. I hope you will read my forthcoming post with interest.